

Research Article | DOI: https://doi.org/10.31579/2835-835X/128
Health seeking behavior for Gout in South Asia: A Systematic Review
- Rizwana Shahid 1*
- Inayat Ullah Amin 2
- Majid Ali Yousafzai 3
- Narjis Zaidi 4
- Rana Muhammad Yasir Bari 5
1 Associate Professor Community Medicine, Rawalpindi Medical University, Pakistan.
2Chief of Research, Pakistan Institute of Development Economics (PIDE), Pakistan.
3Program Director Public Health, Rawalpindi Medical University, Pakistan.
4APWMO, Community Medicine, Rawalpindi Medical University, Pakistan.
5Demonstrator Community Medicine, Rawalpindi Medical University, Pakistan.
*Corresponding Author: Rizwana Shahid, Associate Professor Community Medicine, Rawalpindi Medical University, Pakistan.
Citation: Rizwana Shahid, Inayat U. Amin, Majid A. Yousafzai, Narjis Zaidi, Yasir Bari RM, (2026), Health seeking behavior for Gout in South Asia: A Systematic Review, Clinical Trials and Case Studies, 5(2); DOI:10.31579/2835-835X/128
Copyright: © 2026, Rizwana Shahid. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 March 2026 | Accepted: 03 April 2026 | Published: 10 April 2026
Keywords: acute gouty arthritis; health seeking behavior; south asia; self-management
Abstract
Background: Gout is a non-communicable disease that is raising head in South Asian regions concomitant with rapid lifestyle transition and comorbidities. The current global burden calls for urgent attention to his problem as it may hinder the achievement of health-related Sustainable Development Goals (SDGs). The present study is aimed to determine the heath seeking behavior and barriers to gout treatment and to suggest practical recommendations to policy.
Methods: A systematic literature was carried out by using databases of PubMed, ScienceDirect, Scopus and Pak Medi Net on 24th October 2025. The searching was done with keywords of health seeking behavior, gouty arthritis and South Asia to filter out the eligible studies that were rigorously and methodically evaluated for useful findings.
Results: Only 6 studies fulfilled the eligibility criteria that included 3 quantitative studies, 1 qualitative and 2 systematic reviews. Urate lowering drugs were used by 49.7% or the gout patients while 97.3% were facing financial catastrophe due to this disease. Self-management of gout was done by Indians through traditional methods. The variation in cultural beliefs and food intake was linked with ethnicity. Apart from language and cultural hindrances, financial constraints and distance from healthcare facility were also barriers to seek health care for gout. Healthcare providers also need to be trained for educating and guiding the patients for managing gouty arthritis. There is scarcity of interventional studies on gout in South Asian population.
Conclusion: Gouty arthritis is subjecting the cases to substantial economic burden. Although self-medication prevails but drugs should be prescribed precisely to suppress the symptoms.
Introduction
Gout is commonly prevailing inflammatory arthritis across the globe that not only drastically impairs the quality of life but also preludes to cardio-metabolic comorbidities in case of inadequate management [1]. Its burden has significantly been escalated over the last decade that has mainly been attributed to demographic variations and lifestyle modifications [2]. Moreover, genetic predilection and rapid urbanization seemed to have association with growing gout propensity among South and East Asian residents of the world [3]. According to a meta-analysis, variance in urate levels were chiefly attributed to genetics [4].
A longitudinal survey (2006-2017) carried out in United States elucidated that Asians residing there were having 2.7 times increased likelihood of gout diagnosis compared to those of Caucasians [5]. Acute gouty arthritis is substantially linked with intolerable joint pain that predominantly affects the lower limbs and significantly deteriorates the daily life activities [6]. This ailment has been reported with increased absenteeism and diminished work productivity that are related to amplified economic burden of any society [7]. The accumulation of uric acid crystals in the joints and ligaments can also adversely affect multiple joints including those of upper limbs that in extreme cases may lead to surgical management of the complicated cases [8].
South Asian Region of the globe is subjected to multiple gout related challenges not only due to diverse characteristics of its inhabitants but also due to its exclusive healthcare system where despite need assessment and formulation of robust policies, majority of the public has to avail healthcare facilities by out of pocket payment. The increased reliance on traditional medications for relief of gouty arthritis in our society primarily seems to be due to poor socioeconomic status and inadequate access to the healthcare amenities. Moreover, self-medication, reliance on superstitions and pursuing traditional healers is very commonly practiced by general public for numerous chronic illnesses [9]. The present study aims to determine the health seeking behavior for gouty arthritis and to summarize the treatment patterns of the patients in South Asian regions. This study also intends to map the evidence gaps and to identify health system level barriers and facilitators to appropriate gout care. The resultant financial strains on general public due to this ailment will also be scrutinized. This would prove valuable in guiding suitable recommendations for long-term control of gout.
Despite 22% rising global age-standardized incidence of gout since 1990 [10], it is still among neglected health problems that has been overlooked in various national and international health programs [11]. South Asian countries are subjected to dietary and epidemiological transitions that seems to be a key contributing factor towards escalating incidence of non-communicable diseases [12]. Many reviews have in South Asian countries including Pakistan have emphasized the need to strengthen primary healthcare deliverance to cater the most prevailing non-communicable diseases like diabetes, cancer, chronic respiratory diseases and cardiovascular disorders [13] but gout epidemic has rarely been addressed. Reviewing the health seeking behavior among population residing in South Asian regions pertaining to gout would enable to have an insight not only into their treatment plans by also about severity of this illness. Various aspects of life influencing the gout management would also be brought to the limelight. Appraisal of cultural attitudes towards health, barriers in accessing healthcare and educational gaps would enable the strategic planners and policy makers to develop some tailored management plans for improved healthcare outcomes.
The paper is organized as follows. The next section describes the materials and methods followed by the results in section 3. The results are discussed in section 4 while section 5 concludes the paper.
Materials & Methods
This systematic review has been registered with PROSPERO (ID: CDR420251152433) on 21st September 2025 to avoid duplication of similar reviews. The methodology of our systematic review is given below with various sections that are illustrative of the phases of work done to ensure its authenticity.
Data Sources & Search Strategy
Various electronic databases like PubMed, Medline, Scopus, Google Scholar and ScienceDirect were systematically searched on 24th October 2025. Non-electronic sources were the published books on gout management guideline. The review timeline mentioned for this review was 7th November 2025. Both full text articles and abstracts were reviewed. Our search keywords were 1) acute gouty arthritis 2) health seeking behavior and 3) South Asia that were used with various Boolean operators (AND, OR, NOT). The relevant published articles of Pakistan, India, Bangladesh, Nepal, Sri Lanka, Maldives, Bhutan and Afghanistan were reviewed. Rayyan software was used to avoid data duplication.
Inclusion & Exclusion Criteria
All original studies both observational and interventional studies along with systematic reviews and audits published 2000 onwards in English and based on quantitative or qualitative findings of adult gouty arthritis with respect to health seeking were included. All case reports, editorials, letter to the editors, commentary reviews were excluded. Moreover, grey literature like conference proceedings, thesis / dissertation and data from Non-Government Organizations (NGOs) were also excluded. The review was done in accordance with PRISMA 2020 reporting guidelines [14]. All the published studies based on adult gout cases of aforementioned countries and databases were identified and screened for relevant findings as illustrated below in PRISMA Flow Diagram (Figure 1).
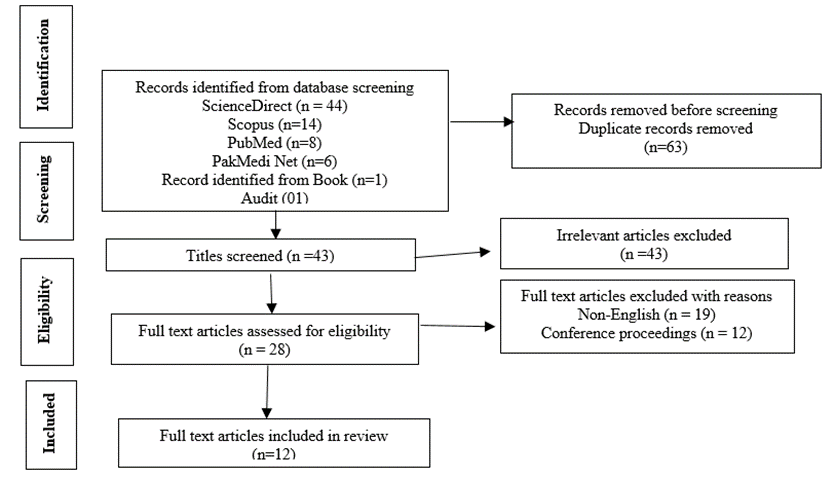
Figure 1: PRISMA Flow Diagram
Data Extraction
The data was extracted from the relevant studies by means of different aforementioned search engines that encompassed various attributes pertaining to the included studies like authors, year of publication, country, title of journal, study design, sample size, demographics (age, gender), types of intervention, results or outcomes in terms of health seeking behavior and delay in treatment. Where information pertaining to certain variables like population characteristics, study population or sampling techniques were uncertain, assumptions were made from the relevant declarations within the searched literature. The risk of bias ascertained in the searched studies by using GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework. The study limitations were also reviewed as given below in Table 1:
Sr# | Author & Year of study | Journal (Title, Volume (Issue), page No. | Country /setting | Study design, Methodology, sample size | Study objectives | Results / key Findings | Bias / Risk assessed |
1 | Ashiq et al., 2022 | Pakistan Journal of Medicine & Dentistry, 11(2), 76-82 | Lahore, Pakistan | Cross-sectional descriptive study was done among 203 gout cases of Lahore. quantitative data collection was done by means of structured questionnaire | To determine knowledge, attitude and practices of gout patients pertaining to their disease |
| According to the literature, gout has strong genetic predisposition but family history of the gout cases was not ruled out. |
2 | Sivasegaran et al., 2023 | Malaysian Family Physician, 18, 72 | Malaysia | A qualitative study was done by purposive sampling among 20 gout cases of which there were 9 Malay, 6 Chinese and 5 Indian. In-depth interviews were taken form study participants pertaining to their experience with gout, type of self-management of gout and variables affecting self-management | To determine perceptions and practices of self-management of gout cases by using Health Belief model as conceptual framework |
|
|
3 | Poudel et al., 2023 | International Journal of Health Sciences and Research, 13(4), 97-105 | Nepal | A cross-sectional descriptive study was done among 221 general public that was residing in a district of Nepal. Health seeking behavior of the study participants was ascertained for various systemic problems including musculoskeletal & neurological disorders.
| To determine the association of health seeking behavior of Nepalese community with selected variables |
| Lack of awareness in the general population was found to be the main obstacle in accessing health care services with absence of financial and family support |
4 | Rai et al., 2018 | Rheumatology, 57, 1282-1292 | Qualitative studies from USA, UK, Netherlands, Australia & New Zealand were included | Total 20 studies were included in systematic review and thematic analysis in accordance with PRISMA 2009 checklist |
|
|
|
5 | Rathore et al., 2022 | Annals of King Edward Medical University, 28(1), 109-118 | Pakistan | 34 articles were reviewed literature-based survey. 31 articles were based on data of Pakistani cases |
| Most (64.5%) of the researches on gout are published as original research work with gross lack of interventional studies |
|
6 | Kanwal et al., 2018 | GSC Biological and Pharmaceutical Sciences, 05(01), 050-055 | Pakistan | Epidemiological data pertaining to gout from United States, United Kingdom, New Zealand, China, Germany and Asian countries was reviewed |
|
|
|
7 | Chaudhary et al., 2022 | World Journal of Advance Healthcare Research, 6(2), 135-141 | Nepal | A prospective study was done among 110 gout cases who were above 20 years of age and non-hospitalized |
|
|
|
8 | Thapa et al., 2015 | Journal of Pharmaceutical Research, 12(4): 902-912 | Nepal | Prospective and descriptive hospital-based study was done among 103 non-hospitalized gout cases |
|
|
|
9 | Parvin et al., 2012 | Journal of Applied Pharmaceutical Science, 2(5), 49-51 | Bangladesh | A cross-sectional multicenter study was done among 150 gout cases who were visiting 4 teaching hospitals of Bangladesh for their treatment. Patients without signs and symptoms of gout were excluded |
|
|
|
10 | Sidha rthan et al., 2020 | Indian Journal of Applied Research, 9(12), 46-48.
| India | An audit was carried out among 350 gout cases 34-82 years of age visiting 3 tertiary care facilities of India |
|
|
|
11 | Paul et al., 2009 | Clinical Journal of Rheumatology, 4(4): 149-152 | Kerala, India | A prospective study was done among 83 gout cases of which 14 lost to follow up. Finally, data was collected from 69 patients who were also subjected to clinical / musculoskeletal examination |
|
|
|
12 | Shah et al., 2023 | Pak J Med Res, 61(4), 150-153. | Peshawar, Pakistan | A descriptive cross-sectional study was done among 323 gout cases who visited a tertiary care hospital of Peshawar. |
|
|
|
Table 1: Summary Table of the Reviewed Articles
Results
A cross-sectional study carried out among gout patients of Lahore revealed involvement of their multiple joints although pain among most (40.39%) of the patients was mild. Majority (49.75%) were using urate lowering medications as prescribed by physicians for relief of symptoms while 15.27% opted intake of prudent diet. About 77.3% of the patients consulted rheumatologists for gouty arthritis. Moreover, gout patients also felt financial strain due to management of this disease [15]. Likewise, a systematic review of gout cases among multiple western countries including those of Asian region elucidated escalating economic burden among Asians due to increased hospital visits for disease management. Moreover, this review emphasized the risk of gout many times greater among postmenopausal cases. As gout cases were consulting the healthcare professionals for multiple comorbid states, so accurate cost estimation for gout treatment is cumbersome [16].
A qualitative study was done among Malay, Chinese and Indian gout cases of a primary care center though in-depth interviews about their perceptions and practices for self-management of gout. Most of them were having self-regulated dietary control. Healthcare professionals can better manage the gout cases individually by appraising the health beliefs and food cultures as there exists diverse ethnic differences among people belonging to different regions of the globe [17]. A cross-sectional study conducted in general population of Nepal not specifically suffering from gout but diagnosed with cardiovascular, respiratory, gastrointestinal and neurological disorders elucidated the mix of health seeking behavior. About 82.4% were dependent on modern medicines while 1.6% sought relief by using complementary and alternative remedies. The chief caveat in the study was lack of adequate knowledge about accessing healthcare facilities with limited resources [18].
A prospective study among Nepalese people was illustrative of high incidence of gout among Brahmins race. Moreover, businessmen specifically those indulged in alcoholism and hypertensive were found to be the main sufferers [19]. A prospective and descriptive study among Nepalese gout patients explicated the intake of purine rich food among more than 80% of the cases. Family history among 38.8% of the gouty arthritis cases. About 53% of the patients were taking combination of urate lowering drugs and estimated monthly cost for treatment of gout was approximately 600 rupees [20]. Devising insurance mechanism for facilitating the gout cases in getting gout medication can be a great instrumental support to reduce the financial burden on general public.
A systematic review and thematic analysis done by using studies from 5 countries across 3 major continents was illustrative of inadequate counseling of the gout patients by healthcare providers for case management. Moreover, scarcity of financial support was also found to be the major hindrance in continuity of healthcare. Training of healthcare workforce is also required to equip them with all essential information for long-term management of the patients by overcoming the language and cultural barriers [21]. A literature-based survey by Rathore et al emphasized the need for more researches on gout as there is negligible research on health seeking behavior for gout in Pakistan. This survey also stressed on planning of clinical trials to compare the efficacy of different hyperuricemic drugs. Such studies would definitely prove beneficial in mitigating the complications of gout cases as gout prevalence is on rise in LMICs due to lifestyle and dietary factors [22].
No doubt, this is an era of non-communicable diseases and hyperuricemia is frequently occurring among obese, diabetics and hypertensive people in the community. A cross-sectional study done among gout cases visiting the four teaching hospitals of Bangladesh elucidated that obese individuals have greater predisposition to gout as excessive deposition of adipose tissue is accompanied with insulin resistance, which impairs uric acid clearance. More than half of the gouty arthritis cases were hypertensive. A strange finding of that multicenter study was linkage of viral hepatitis with gout that should meticulously be investigated among diverse ethnicities for establishing the association [23]. A prospective study carried out among 83 gout cases of Kerala state emphasized the impregnation of uric acid crystal in the first metatarsophalangeal joint of about 91.3% gout cases. However, 10% patients reported involvement of their multiple joints and their mean serum uric acid was 9.2 mg/dl. Apart from history of hypertension and obesity, 16% of the gout patients were found to have renal calculi although none of them had renal failure. This study seemed to be quite authentic as in addition to relying on the medical history of the cases, their musculoskeletal examination was also done that is valuable in distinguishing inflammatory, degenerative and metabolic conditions [24].
A study among gout cases of Peshawar also revealed the occurrence of obesity and hypertension among more than 60% of the gout patients. Moreover, vitamin D deficiency was also identified significantly in addition to other arthropathies [25]. A multicenter study done among 350 gouty arthritis cases of India revealed the prescription of NSAIDs and steroids alone or in combination for relief of the arthralgia and arthritis [26]. Although these medications are useful in reducing joint damage and improving joint mobility; yet, lifestyle modification for reversing obesity and hypertension can help a great deal to prevent the complications of various metabolic disorders.
Discussion
Most of the studies on gout in Asian countries have been carried out to delineate the risk factors with an intent to diminish the frequency of cases. Likewise, as systematic review was done during 1990-2021 that was primarily aimed to determine the disparities in the rise of gout incidence and risk factors among regions with varied Socio-Demographic Index (SDI) [27]. Health seeking behavior of any society is driven by its physical, socio-economic, cultural and political traits. Hence, adequate appraisal of these traits of any community is necessitated for arranging health promotional campaigns through intersectoral collaboration regarding the rising propensity of gout, preventive measures against this disease and need to consult physician or rheumatologist for treatment [28]. Limited studies are available on health seeking behavior of gout cases from South Asian countries that reflects the extensive research gap due to weak surveillance system. Strengthening the health surveillance system nationwide is high priority need to detect high risk population and to track geographic hotspots for timely interventions.
The global incidence of gout cases is projected to rise up to 70% by 2050 compared to those reported in 2020. Being unexplored and inconclusive disease, gout should methodically be studied in low-middle- income countries to predict the likelihood of resultant disabilities [29]. Specific and evidence-based guidelines have been formulated for clinical appraisal and management of the gout by American College of Rheumatology [30] and European Alliance of Associations for Rheumatology [31]. The guidelines for gout management in developing or third world countries have recently been established with great emphasis on carrying out interventional studies to mitigate the frequency of disabilities as financial constraints make it impossible for Lower-Middle-Income Countries (LMICs) to manage the resultant joint deformities and impaired quality of life [32]. This latest formulation of gout management guidelines for developing nations is descriptive of enhanced focus on this disease like other non-communicable diseases as this is the need of time to curb its mushroom growth. This will be a small but remarkable step towards achieving health related Sustainable Development Goals that are to be attained by all countries by 2030.
A systematic review and meta-analysis in India emphasized the need of determining health seeking behavior for non-communicable diseases due to their steep rise worldwide and fear of confrontation with horrible and irreversible consequences. It is imperative to understand the significance of socio-economic and cultural factors in addition to attributes of healthcare system that may influence the access of general public to healthcare services [33]. A narrative review underscored the need to empower the Community Health Workers (CHWs) in South Asian regions to ensure universal health coverage through health counselling and community-based services. These are mainly targeted to improve the maternal, neonatal and child health due to suboptimal reproductive health indicators. Integrating CHWs into Primary Health Care would really help to lessen the frequency of non-communicable diseases through health education and life style modification [34]. Moreover, home-to-home visits by CHWs will also enable to garner data about health seeking practices for such silent epidemics.
Catering the healthcare needs and existing problems of a common man intelligently through providing desired clinical support and acquainting them with relevant e-Health services is also a cost-effective approach that would enable to get real-world statistical image of gout [35]. Target 3.4 in SDGs is meant to reduce premature mortality from commonly presenting non-communicable diseases by one third till 2030 [36]. Although gout has not been prioritized for stringent prevention and control, but it may result in premature death in co-existence with cardiovascular and renal related comorbidities [37]. The qualitative studies on gout by gathering information about lived experiences, health seeking behavior and barriers to treatment among South Asian patients would really be valuable to grasp the truth as biomedical quantitative data alone is insufficient to perceive the gravity of this health problem. Fulfilling this widespread research gap would definitely ensure equitable policy making to facilitate marginalized and vulnerable people of the society.
Conclusion & Recommendations
There is scarcity of data on health seeking behavior of gout patients in South Asian countries. Strengthening the role of Community Health Workers by incentivizing them and incorporating e-health services either by sending health messages at doorstep or by practicing Telemedicine can be advantageous in developing rapport with gout cases and determining their health seeking behavior. Detailed history taking along with clinical assessment of the patients is imperative for meticulous prescription of drugs.
There is need to explore the grey literature pertaining to gout in order to get an insight about Out of Pocket (OOP) expenditure for this disease as SDG 3.8 is directly addressing the achievement of Universal Health Coverage (UHC) by 2030 in all United Nations member states. There is substantial dearth of qualitative studies regarding health seeking behavior for gout in South Asian countries. Although prevalence of gout in South Asia is very low; yet discussion with the patients will uncover the pain severity in extremities associated with gout along with functional limitations and emotional distress.
Conflicts Of Interest: The authors declared no conflict of interest.
Source Of Funding: The author(s) received no financial support for the research, authorship and or publication of this article.
References
- Asghari KM, Zahmatyar M, Seyedi F, Motamedi A, Zolfi M, et al. (2024).Gout: global epidemiology, risk factors, comorbidities and complications: A narrative review. BMC Musculoskelet Disord 25(1): 1047.
View at Publisher | View at Google Scholar - Wang U, Li W, Wu H, Han Y, Wu H, et al. (2023). Global status and trends in gout research from 2012 to 2021: a bibliometric and visual analysis. Clin Rheumatol 42(5): 1371-1388.
View at Publisher | View at Google Scholar - Butler F, Alghubayshi A, Roman Y. et al. (2021). The Epidemiology and Genetics of Hyperuricemia and Gout across Major Racial Groups: A Literature Review and Population Genetics Secondary Database Analysis. J Pers Med 11(3): 231.
View at Publisher | View at Google Scholar - Major TJ, Topless RK, Dalbeth N, Merriman TR. et al. (2018). Evaluation of diet wide contribution to serum urate levels: meta-analysis of population-based cohorts. BMJ 363: k3951.
View at Publisher | View at Google Scholar - Chen-Xu M, Yokose C, Rai SK, Pillinger MH, Choi HK. et al. (2019). Contemporary Prevalence of Gout and Hyperuricemia in the United States and Decadal Trends: The National Health and Nutrition Examination Survey, 2007-2016. Arthritis Rheumatol 71(6): 991-999.
View at Publisher | View at Google Scholar - Dalbeth N, Merriman TR, Stamp LK. Gout. The Lancet 2016; 388(10055): 2039-2052.
View at Publisher | View at Google Scholar - Kleinman NL, Brook RA, Patel PA, Melkonian AK, Brizee TJ, et al. (2007). The impact of Gout on work absence and productivity. Value Health 10(4): 231-237.
View at Publisher | View at Google Scholar - Yokose C, Dalbeth N, Wei J, Nicolaou S, Simeone FJ, et al. (2020). Radiologic evidence of symmetric and polyarticular monosodium urate crystal deposition in gout - A cluster pattern analysis of dual-energy CT. Semin Arthritis Rheum 50(1): 54-58.
View at Publisher | View at Google Scholar - Anwar M, Green J, Norris P. et al. (2012). Health-seeking behaviour in Pakistan: A narrative review of the existing literature. Public Health 126(6): 507-517.
View at Publisher | View at Google Scholar - Cross M, Ong KL, Culbreth GT, Steinmetz JD, Cousin E, et al. (2024). Global, regional, and national burden of gout, 1990-2020, and projections to 2050: A systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol 6(8): e507-e517.
View at Publisher | View at Google Scholar - Bhattacharya S, Heidler P, Varshney S. et al. (2023). Incorporating neglected non-communicable diseases into the national health program-A review. Front Public Health 10: 1093170.
View at Publisher | View at Google Scholar - Bishwajit G. et al. (2015). Nutrition transition in South Asia: the emergence of non-communicable chronic diseases. F1000Res 2015; 4: 8.
View at Publisher | View at Google Scholar - Ahmed SM, Krishnan A, Karim O, Shafique K, Nahir N; et al. (2024). Delivering non-communicable disease services through primary health care in selected South Asian countries: Are health systems prepared? Primary Health Care in South Asia 12(10): E1706-E1719.
View at Publisher | View at Google Scholar - Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, et al. (2021). The PRISMA 2020 Statement: An updated guideline for reporting systematic reviews. International Journal of Surgery 88: 105906.
View at Publisher | View at Google Scholar - Ashiq K, Bajwa MA, Ashiq S, Qayyum M, Yasmeen A, et al. (2022). Knowledge, attitude and practices assessment of the Gout patients residing in Lahore, Pakistan. Pak J Med Dent 11(2): 76-82.
View at Publisher | View at Google Scholar - Kanwal A, Abida L, Sana A, Ahlam S. et al. (2018). A systematic review on the prevalence, pathophysiology, diagnosis, management and treatment of gout (2007-2018). GSC Biological and Pharmaceutical Sciences 05(01): 050-055.
View at Publisher | View at Google Scholar - Sivasegaran S, Hanafi NSH. et al. (2023). Perceptions and practices of self-management among adult patients with gout at a primary care clinic: A qualitative study. Malays Fam Physician 18: 72.
View at Publisher | View at Google Scholar - Poudel S, KCP, Mandal R, Rana S. et al. (2023). Health seeking behaviour of community people in Lalitpur District of Nepal. International Journal of Health Sciences and Research 13(4): 97-105.
View at Publisher | View at Google Scholar - Chaudhary MK, Chaudhary K, Tharu KC, Jamarkattel N, Nepali S et al. (2022). Prescription pattern of gout: A prospective study. World Journal of Advance Healthcare Research 6(2): 135-141.
View at Publisher | View at Google Scholar - Thapa S, Upadhya N, Gautam S. et al. (2015). Study of risk factor, prescription pattern and cost estimation of acute gout in private hospital. Journal of Pharmaceutical Research 12(4): 902-912.
View at Publisher | View at Google Scholar - Rai SR, Choi HK, Choi SHJ, Townsend AF, Shojania K, et al. (2022). De Vera MA. Key barriers to gout care: A systematic review and thematic synthesis of qualitative studies. Rheumatology57: 1282-1292.
View at Publisher | View at Google Scholar - Rathore FA, Ilyas A, Farooq F. et al. (2022).The analysis of published research on gout and hyperuricemia from Pakistan in National Biomedical Literature. Annals of King Edward Medical University Jan-Mar 28(01): 109-118.
View at Publisher | View at Google Scholar - Parvin MN, Chowdhury SA, Islam SMA, Uddin R. et al. (2012). Pattern and treatment of Gout in Bangladesh: A hospital-based survey at Dhaka city, Bangladesh. Journal of Applied Pharmaceutical Science 2(5): 49-51.
View at Publisher | View at Google Scholar - Paul BJ, Rahman TM, Sudheesh T. et al. (2009). Clinical study of gout in South Kerala. Clinical Journal of Rheumatology 4(4): 149-152.
View at Publisher | View at Google Scholar - Shah MS, Sajjad MM, Khan S, Khan Z. et al. (2023). Co-morbidities in patients presenting with gout at tertiary care hospital Peshawar, A cross sectional study, 2021 Pakistan. Pak J Med Res 61(4): 150-153.
View at Publisher | View at Google Scholar - Sidharthan N, Singhal A, Nazarin R, Unni M, Lalwani C, et al. (2020). Prevalent practices in the management of gout: A three centre study from India. Indian Journal of Applied Research 9(12): 46-48.
View at Publisher | View at Google Scholar - Yang F, Chen R, Xiong J, Wang W, Yu P, et al. (2025). The disease burden of gout in Asian countries and regions from 1990 to 2021, risk factors and forecast analysis: A systematic study of Asian disease burden in 2021, PLoS One 20(7): e0328543.
View at Publisher | View at Google Scholar - Shaikh BT, Hatcher J.et al. (2005). Health seeking behavior and health service utilization in Pakistan: challenging the policy makers. J Public Health (Oxf) 27(1): 49-54.
View at Publisher | View at Google Scholar - Ong L, Vos T, Culbreth G, Steinmetz J, Cousin E, et al. (2024). Global, regional, and national burden of gout, 1990-2020, and projections to 2050. The Lancet Rheumatology 6(8): E507-E517.
View at Publisher | View at Google Scholar - FitzGerald JD, Dalbet N, Mikuls T, Brignardello-Petersen R, Guyatt G, et al. (2020). American College of Rheumatology guideline for the management of gout. Arthritis Care & Rheumatology 72(6): 879-895.
View at Publisher | View at Google Scholar - Russell MD, Rutherford AI, Ellis B, Norton S, Douiri A, et al. (2022). Management of gout following 2016/2017 European (EULAR) and British (BSR) Guidelines: An interrupted time-series analysis in the United Kingdom. The Lancet Regional Health – Europe 18(4): 100416.
View at Publisher | View at Google Scholar - (2024). Al-Worafi YM. Gout and hyperuricemia management in developing countries. In Book: Handbook of Medical and Health Sciences in Developing countries. 1-44, Germany: Springer.
View at Publisher | View at Google Scholar - Haridoss M, Nandi D, Lenin RR, John SP, Anantharaman VV, (2025). Health-seeking behavior and its determinants for non-communicable diseases in India – A systematic review and meta-analysis. Front Public Health 13: 1580824.
View at Publisher | View at Google Scholar - Shrestha P, Afsana K, Weerasinghe MC, Perry HB, Joshi H, et al. (2024). Strengthening primary health care through community health workers in South Asia. The Lancet Regional Health -Southeast Asia 2024; 28: 100463.
View at Publisher | View at Google Scholar - van der Ven J, van den Bemt BJF, Ariaans F, Vriezekolk JE, Flendrie M, et al. (2024).Support needs of gout patients and suitability of eHealth to address these needs. Rheumatology Advances in Practice 2024; 8(4): rkae125.
View at Publisher | View at Google Scholar - (2015).World Health Organization. Targets of Sustainable Development Goal 3.
View at Publisher | View at Google Scholar - Oka P, Chong WM, Ng DX, Aau WK, Tan NC. (2023). Epidemiology and risk factors associated with gout control among Adult Asians: A real-world retrospective cohort study. Front Med 10: 1253839.
View at Publisher | View at Google Scholar
