

Case report | DOI: https://doi.org/10.31579/2835-8325/045
Growing Kidney Stones Disease in Teen age Girls! Who is responsible? School or State! Urgent Need of providing WASH facilities in Schools & Colleges in India
- K. Suresh 1*
Family Physician & Public Health Consultant, Bengaluru
*Corresponding Author: K. Suresh, Family Physician & Public Health Consultant, Bengaluru
Citation: K. Suresh, (2023), Growing Kidney Stones Disease in Teen age Girls! Who is responsible? School or State! Urgent Need of providing WASH facilities in Schools & Colleges in India, Clinical Research and Clinical Reports, 3(1); DOI:10.31579/2835-8325/045
Copyright: © 2023, K. Suresh. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 October 2023 | Accepted: 30 October 2023 | Published: 21 November 2023
Keywords: kidney, urolithiasis, kidney stone disease (ksd); glomerular filtration rate (gfr); chronic kidney disease (ckd); extracorporeal shock wave lithotripsy (eswl); ureteroscopy
Abstract
Kidney Stone formation has been directly associated with a lack of fluid intake and is by far one of the most common causes. Kidney Stone Disease incidence in teenagers especially girls has been increasing in the last decade, due to restricted water consumption, to minimize the need for use of washroom facilities either due to dirty toilets or lack of toilets in the schools and colleges. Restriction of fluids leads to less than 1.5 liters of urinary output per 24 hours. Concentrated urinary output facilitates stone formation in the kidneys. Kidney stone disease (KSD) is a type of solid hard mass formation by aggregation of tiny particles in the kidneys or ureters increasing the risk of chronic kidney disease (CKD). This leads to a progressive decrease in Glomerular Filtration Rate (GFR) and early setting of end stage renal disease (ESRD).
Calcium oxalate, forms Randall's plaque on the renal papillary surfaces, is the most frequent type of kidney stone. VDR Fok1 is a risk factor for renal stone formation and could cause the formation of renal stones through the mechanism of crystal induction and crystallization in the urine. While among adults two third cases are reported among men when compared to 1/3 in women, in teenagers this gender bias is not that explicit.
Feeling like you need to urinate all the time, even if you just finished. Only having a small amount of urine when you urinate. Urinating more frequently than you usually do are the most common symptoms young girls fail to recognize or report to their parents or even teachers. It’s “States Responsibility” to provide school and College students access to clean and appropriate toilets, functioning handwashing facilities with soap, sufficient and safe drinking water and promote developing adequate general and menstrual hygiene skills among girls. Let Schools Learn and teach about the equal division of hygiene-related tasks (Using and cleaning of toilets, fetching and filtering or boiling water, taking care of sick people) between boys & girls.
Globally most KSD cases are managed by conservative approaches of increased fluids, antibiotics, muscle relaxants and pain-relieving medicines, especially among first time sufferers. Sometimes non-invasive techniques like Lithotripsy or other surgical approaches may be required.
This article is based on an uncommon case in a teenaged girl, due to restricted water consumption, for want of rest room facilities in the schools where she spends about 6 hours each day for 6 days a week. It was managed successfully by conservative approach and the girl and parents educated about the need and urgency of keep oneself well hydrated and better dietary practices.to avoid the recurrence. Having guided this case remotely, the author researched the global trends of kidney stones in teenagers and collated the literature.
Materials & Methods
This article is based on a case of 16-year-old girl’s family getting emergency call from the school and the girl in sudden and severe renal colic, rushed to a pediatrician and managed well conservatively after due investigations including CT scan of abdomen and Pelvis. Though the girl suffered for about 2 weeks has been free from the KSD colic since November 2022. The global literature review indicates that the KSD in adolescents is increasing but not yet fully understood. In India low water intake and sometimes increased intake of sugary fluids like Pepsi, Coke etc. by urban teenagers appear to be trigger factors apart from dietary fallacies.
Introduction
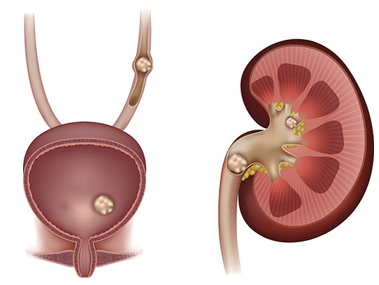
Kidney stone disease (KSD) is a type of solid hard mass formation by aggregation of tiny particles in the kidneys, then moving down anywhere in urinary tract system increasing the risk of chronic kidney disease (CKD). This leads to a progressive decrease in Glomerular Filtration Rate (GFR) and early setting of end stage renal disease (ESRD). Calcium oxalate, forms Randall's plaque on the renal papillary surfaces, is the most frequent type of kidney stone. VDR Fok1 is a risk factor for renal stone formation and could cause the formation of renal stones through the mechanism of crystal induction and crystallization in the urine [1,2]
Kidney stones have become more common in teens over the past decade [3]. One factor all doctors agree on is that today’s teens aren’t drinking enough water. Kidney stones are made up of minerals from our diet. Our body uses what it needs, and the rest goes out in our urine. To form crystals that turn into stones, those minerals need to find each other. The less we drink, the less urine we produce, and the more likely those things are to find each other and form stones if there is not enough urinary output per day to flush out. More water in the urine helps stop stones from forming. Most of the girls pass less than 1.5 liters of urine per day in Inda. Stones typically form in the kidney or ureter, and rarely form in the bladder.
Nationally, there’s been a 3-4-fold increase among teenagers. We’re seeing more cases partly because of better diagnostic tools like a CT of the patient’s abdomen, and the bigger contributors to the increase in kidney stones are excess salt and sugars in ready to eat foods. Teenagers should consume much less based on their size (1200-1400 mg).
Stone formation is mostly attributed to two mechanisms: (1) renal calcium leak, excessive absorption, bone resorption/formation imbalance; and (2) mineralization. Daily fluids consumption and dietary factors have been widely recognized as the primary risk factors of kidney stone formation [5]. On the other hand, the parathyroid hormone primarily modulates calcium balance. Vitamin D receptor (VDR) regulates calcium homeostasis by affecting bone resorption and calcium absorption. CLDN-14, a tight junction
protein, decreases Ca2+ permeability, whereas matrix gla protein (MGP) regulates calcification [4]. Secreted Phosphoprotein 1 (SPP1) prevents renal stone formation by decreasing the aggregation of crystals and binding to the renal epithelial cells. These genes are significantly associated with KSD in the Indian population [5]. These are the reasons for the initial stone formation in the form of insoluble calcium oxalate or calcium phosphate crystals.
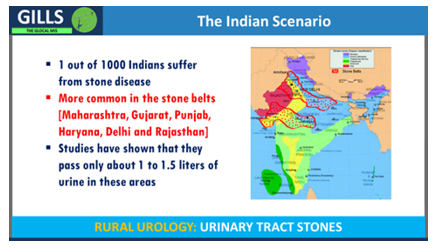
Magnitude of the problem: In the context of Rural India, KSD is reported to be prone among 12% of the total population. Of this half of the population are severely affected by renal damage, leading to a loss of kidneys [4]. Inter-region differences are observed with the country as in South India, a few percentages reported Urolithiasis, as compared to North India, where a steep 15% of the population report KSD [5,6,7]. The kidney stone belt in India includes Maharashtra, Gujarat, Rajasthan, Punjab, Haryana, Delhi, Madhya Pradesh, Bihar, and West Bengal [4] where the weather is very hot for about 5-6 months of every year leading to dehydration and consequent KSD formation. Overall, 2% of the population have stone in their lifetime. While 12% of men suffer from kidney stone by age of 70, only 5% of women will suffer from kidney stone by the same age. Higher BMI is also associated with KSD [14]. Nearly 50% have recurrence within 5-10 yrs. Highest incidence of kidney stone is in 30-45 years of age group, and incidence declines after age of 50. 7-10 of every 1000 hospital admission is of renal stone [4].
Most kidney stones are crystalline in structure, most of the time (80%) they are composed of calcium oxalate and calcium phosphate. Of the remaining 20%, Uric acid (9%), Struvite (10%) and cystine (1%) contribute. Uric acid stones form when the level of uric acid in the urine is too high and the precipitate solidifies. Struvite stones are a result of kidney infections, and cystine is due to a kidney issue. A kidney stone can move in the kidney and give a bad ache. When it starts to move down the ureter to the bladder the ureter/s goes into spasm the pain hits suddenly and severely. As the ureter is about 3-4mm in diameter, stones of that size or smaller usually pass without symptoms, but larger stones get stuck and can create a great deal of pain as our body tries to push them out [5,7,8].
A misconception is that drinking too much milk can cause kidney stones. A recent study shows that nutritional calcium intake does not influence kidney stones unless consumed in extreme amounts [10].
Most KSD cases are managed by conservative approaches of increased fluids and antibiotics, muscle relaxants and pain-relieving medicines. AYUSH treatments are also popular in India. Less than 10% of first time KSD cases are subjected to Extracorporeal Shock Wave Lithotripsy (ESWL), and rarely Ureteroscopy, Percutaneous Nephrolithotomy (PCNL) are used. Exceptionally rarely Retrograde intra renal surgery (RIRS) and Mini percutaneous nephrolithotomy is reported if the size of the kidney stone is more than 8-10 mm [3].
Case Report
The class teacher of Swati, a 16-year-old girl studying in class 10, called on 12 October 2022, in Hubballi, Karnataka asking the mother to come to school and fetch her to a doctor as she was in severe abdominal pain. On arrival the mother saw her daughter in severe pain in back on Left side groin, nausea, and vomiting. She also complained of burning while peeing or bloody urine half an hour ago.
She was taken to a pediatrician who got done urine and blood tests.
- Key Urine test report indicated, yellow colored urine with PH of 5.0, 1.015 specific gravity, blood in urine and microscopic examination showed 3-5 epithelial cells, 80-10 RBCs and plenty of pus cells / per high power field (HPF)
- Blood tests showed absolute leucocyte count of 3800 (normal range 1-3K), Blood group A RH+,
- Ultrasonography of the abdomen and Pelvis clearly showed i) Left renal calculus, ii) left uretero-renal-hydronephrosis iii) about 3-4 mm calculi in mid-pole and another 5 mm calculi in proximal ureter about 3.5 Cm from PUJ. iv) Urinary bladder was normal with no calculi. v) Few enlarged mesenteric lymph nodes.
- She was given 4 pints of IV fluids Glucose saline) and advised to take i) Tablet Nitro best (contains Nitrofurantoin an urinary Antibiotics) 100mg twice a day for 5 days ii) Tab Dytor plus (contains spironolactone and torsemide, which are diuretics removing the excess water) 10mg half tablet in the morning and afternoon iii) Tab Veltman 0.4 mg (It works by relaxing the muscles around the bladder exit in the night) in the night for 10 days iv) Syrup Uro-pot 10 ml (a vitamin, for the treatment and prevention of vitamin B6 deficiency) three time a day for 10 days v) Tab Dolowin (Aceclofenac and Paracetamol combination for relieving pain and inflammation )10 mg twice a day for 5 days vi) Tab Pantin 40 mg ( to treat gastroesophageal reflux disease (GERD) and reflux esophagitis) morning and night for 10 days.
This case represents a rare risk for young school going girl restricting water intake for 6-8 hours they spend in schools for want of toilets or clean toilet facilities in most rural schools and some urban schools.
Discussions
Virtually all stones are formed in the kidneys, initially as small particles. These particles grow within the kidney to varying sizes, often filling up the whole kidney as a branched stone. Sometimes they move out of the kidney when relatively small, and then migrate down the ureter into the bladder. Some stones less than 5 mm in size pass out spontaneously, but occasionally they migrate down the ureter & they may block the ureter causing obstruction to the flow of urine. This results in pain, which may be very severe (ureteric colic). Nausea and vomiting can also be associated with the colic pain. Some stones reach the bladder, and lodge there, growing larger and larger. Rarely the stones block the urethra causing a painful retention of urine [1,4].
A study of 153,000 pediatric, as well as adult patients, treated for kidney stones between 1997-2012 inferred an annual incidence increase by 16% and the largest incidence was among 15 to 19-year-olds. The childhood cumulative risk for kidney stones was the same for both boys (90%) as well as girls (87%). The lifetime risk for kidney stones increased for women from 10.5% to 15.2% while it remained constant for men - 23% [9].
There are two main reasons why teenagers develop stones. The first is genetics, that contributes to only 5% of children that develop kidney stones. The more prevalent causes that can increase the risk for kidney stones are environmental contributors such as fluid consumption, nutrition, and geographic location. Any salt that is consumed is absorbed in the body and finds its way into the urine. For simplicity, salt basically drags calcium to the urine and too much calcium can cause hard deposits to develop. Hot weather, school /work environment and/or dehydration can promote the development of kidney stones. For example, in rural India an increase in kidney stones in high school girls is noticed as they restrict water intake for want of rest room facilities. The incidence of kidney stones decreases significantly simply by drinking more liquids [11]
There are many types of kidney stones, but the most common among Indian teens are calcium oxalate and calcium phosphate stones. Less often, stones are made of uric acid, and cystine an amino acid, or the mineral struvite. Kidney stones vary in size, with most about 1/8-1/4 inch. Finding out what the stone is made of can help the doctor find ways to stop more stones from forming. Apart from family tendency to form stones, low urine output from not drinking enough fluid, a diet high in salt, meat, and low in fruits and vegetables, certain medicines, seizure drug topiramate, or the blood pressure drug furosemide, which removes excess water from the body are the main causes of stone formation. In Indian school girls, lack of clean toilet facilities in the schools forces the girl students, to not to drink water for hydration leading to the kidney stones. Stones can form in a teenager’s kidney without causing symptoms for a long time, but when the stone starts to move down the urinary tract through the ureter, it can cause symptoms to appear. Most common symptoms like sudden, severe pain in back or side, nausea and vomiting, groin pain, severe stomach pain only along with burning or pain while peeing or even blood in urine (hematuria). If not attended fever due to urinary tract infection may show up [5,6,7,8].
A case-control prospective study conducted in Guru Teg Bahadur (GTB) Hospital, a tertiary care facility in Delhi with 30 cases and 30 controls. Patients visiting the department of surgery between November 2011 and April 2013 were enrolled in the study. Cases were defined as patients with renal stones diagnosed based on history and radiological investigations. Controls were selected from the patients admitted to the department of surgery for reasons other than renal stones. Metal levels were analyzed by an atomic absorption spectrophotometer at Delhi University. The vitamin D receptor gene was measured using genomic DNA. Horizontal agarose gel electrophoresis was used for the quantification of genomic DNA. The results indicated a higher level of stress prevalent among cases (63%) compared to controls (36%). Nearly 83% of cases had the ff allele of the Vitamin D receptor gene compared to 46% of controls. The median arsenic and lead levels were higher among cases compared to controls. In the unadjusted model of logistic regression, study found that stressed patients had three times higher odds of developing renal stones compared to non-stressed patients (OR (95% CI): 2.98 (1.04-8.52); p=0.04). Similarly, patients with higher blood concentrations of arsenic and lead had higher odds of developing renal stones compared to controls. There was a definitive role of heavy metals, including lead, cadmium, and arsenic, seen with renal stones. A significant association was seen between the ff allele of VDR polymorphism (Fok1 enzymes) and patients with renal stones. Other parameters, including male and stress factors, seem to have an important role in renal stone formation [5].
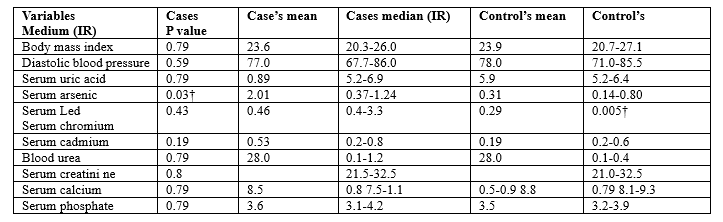
Note: IR= Interquartile range
A significant difference in average serum levels of Serum Arsenic and Serum led was observed between cases and controls.
It has been observed that genetic polymorphism of vitamin D receptor (VDR), Klotho, and chloride voltage-gated channels (CLCN) genes have a role in the formation of kidney stones.
A study published in 2021 also showed that the mean age of renal stone occurrence was 21-40 years [4]. A retrospective study on 435 patients who visited the urology outpatient clinic in Dehradun, India, between 2005 and 2018 showed a three times higher prevalence of renal stones in males than in females. It was also suggested that this prevalence might be due to high levels of testosterone in males [5]. Another study done by Lohiya et al. in northern India, which included 435 renal stones patients, demonstrated a high prevalence of 1.5 times mores tones in males, than in females [7]. A study done by Semins et al. in approximately 3.4 million insured individuals during a five-year period (2002 to 2006) concluded that the occurrence of renal stones is directly proportional to age, and the disease was twice more common in males as compared to females [7].
Food intake plays a pivotal role in human growth, constituting 45% of the global economy and wellbeing in general. Diet is an integral part of renal accumulation and thus filtration, which in turn affects the absorption and bodily homeostasis of renal stone occurrence. Food patterns are among the major factors for renal stone formation, and stone material deposition can be managed by regulating food intake. In the context of the Indian diet, the color-rich food of Rajasthan, to the spicy food of Punjab, and slightly sweet & oil-based food of Gujarat, to the southern, slightly sour seafood. Consumption of animal proteins increases in urinary calcium excretion, with a consequent reduction in urinary pH and citrate excretion, which are the basis of stone formation [8].
Kidney stones Management in India:
Based on a pluralistic approach to health care, India offers a range of medical treatment modalities to its population. Though reported case was managed by allopathy system practitioner for completion of traditionally followed treatment of three main streams of therapies are:
1. Allopathy:
i) Drinking water: Increasing water intake can help flush out small stones from the urinary tract. Consuming maximum amount of water is the key intervention for passing stones, of even 6-8 mm as they get flushed.
ii) Do not drink fluids like a) Dark colas and other carbonated drinks as they are made of chemicals and high amounts of sugar, b) Store-bought fruit juices iii) Coffee iv) Black Tea and v) Alcohol.
iii) Pain management: Over-the-counter pain relievers such as ibuprofen and acetaminophen can be taken to manage the pain caused by kidney stones.
iv) Medications: Some medications such as alpha-blockers can help relax the muscles in the ureter and allow small stones to pass more easily.
v) Extracorporeal Shock Wave Lithotripsy (ESWL): In this procedure, shock waves are used to break the kidney stones into smaller pieces that can be passed in urine.
vi) Ureteroscopy: A small scope is passed through the urethra and bladder and into the ureter to remove or break up the stone.
vii) Percutaneous Nephrolithotomy (PCNL): This procedure involves making a small incision in the back and using a scope to remove the kidney stones.
viii) Retrograde intra renal surgery (RIRS) - In this procedure, a flexible ureteroscope is passed into the kidney and laser is used to fragment stones. Fragments can be removed using small baskets.
ix) Mini PCNL or Mini percutaneous nephrolithotomy - A small keyhole is made in the kidney and stones are seen using a mini nephroscope, fragmented and removed.
2. Ayurvedic system: Ayurveda advocates consumption of Fine wheat flour (Maida), Oatmeal, Bran, Amla, Black grapes, Kiwi, Chikoo eat sugarcane with cumin seeds or honey, fennel seeds, coriander, and Strawberries. It also advises start consuming Barley water (morning and evening), Drinking sugar cane juice mixed with cardamom twice a day on an empty stomach, sugarcane with Tulsi (basil) seeds and milk, Buttermilk, tender Coconut water (in the morning), Lemon water, sweet lime juice (once a day, preferably after lunch) and Pumpkin soup in moderation, to manage recurrence of a kidney stones. The best, easiest, quick, and less painful way to remove kidney/bladder/ureter stone is to have kulthi dals (horse gram) water in empty or atleast half empty stomach. Boil 2–3 eating spoon of dal(pulse) in around 2 glasses of water till it gets totally colored and keep drinking 3-4 times a day [15].
Ayurvedic herbal medicines used include Punarnava (Boerhaavia Diffusa), Shigru (Moringa Oleifera), Varuna (Crataeva nurvala), Kantkari (Solanum xanthocarpum), Kushmanda seeds (Benincasa hispida), Pashanabheda (Bergenia ligulata), Coriander (Coriandrum Sativum), Jasmine (Jasminum auriculatum), Bakul (Mimusops Elengi) andKerala Ayurveda’s herbal formulation, Punarnavasava [13].
Homeopathy Treatment [16]:
i) Arsenicum: This homeopathy medicine is used in all stages of CKD and is one of the best remedies. Taking aconite produces mucus and the patient gets relief.
ii) Belladonna: Belladonna is the ideal homeopathic remedy for treating inflammation of the kidneys accompanied by piercing or burning pain in the lumbar region of the kidney. The pain reappears repeatedly with increased intensity each time.
iii) Apis mellifica: This homeopathic medicine is used when there are dull aches in the kidney, reduced urination, and micturition. The urine contains albumen in high levels and RBCs, if the patient feels drowsy or any skin eruption occurs.
iv) Aurum muriaticum: This homeopathic medicine is used to cure renal diseases such as Morbus bright caused by gout or from syphilis.
v) Cantharis: medicine is used in nephritis, with a cutting pain in the lumbar region, or the urine contains blood, and the flow is in the form of drops.
vi) Conavallaria: Conavallaria is used in case of nephritis occurring due to heart disorders like mitral insufficiency.
Conclusion
- In India 12% of men and only 5% of women suffer from kidney stone by the age of 70 years
- Highest incidence of kidney stone is in 30-45 years, and incidence declines after age of 50.
- KSD in teenagers has been increasing in the last decade, the main reason being restricted fluids intake, leading to less than 1.5 liters of urinary output per 24 hours.
- Water intake is restricted by girls for want of rest rooms in schools and junior colleges in rural areas & habit of consuming aerated drinks like Pepsi, Coke, etc. in urban areas.
- Nearly 50% have recurrence within 5-10 yrs.
- Provision of drinking water and restrooms in educational institutes and garment factories needs to be prioritized.
- Most KSD cases are managed by conservative approaches of increased fluids and pain-relieving medicine and antibiotics. AYUSH treatments are also popular in India.
- A child that has developed kidney stones is at greater risk for developing additional stones in the future. Drinking more fluids, eating a healthily diet, low salt consumption, physical exercises, are key to prevent recurrence.
- It’s States Responsibility to provide school and College students access to clean and appropriate toilets, functioning handwashing facilities with soap, sufficient and safe drinking water and promote developing adequate general and menstrual hygiene skills among girls.
- School teachers must monitor and help requisite quality hygiene skills and take-home messages of good hygiene practices.
- Let Schools Learn about the equal division of hygiene-related tasks (Using and cleaning of toilets, fetching & filtering or boiling water, taking care of sick people) between boys & girls.
References
- Kidney stones - Symptoms and causes - Mayo Clinic [Internet]. [cited 2021 Aug 4].
View at Publisher | View at Google Scholar - Kidney Stone-Bangalore - Fairfield Health [Internet]. [cited 2021 Aug 10].
View at Publisher | View at Google Scholar - Kidney Stones in Children and Teens.
View at Publisher | View at Google Scholar - Rural Surgery Urinary Tract Stones, J. Gnanaraj.
View at Publisher | View at Google Scholar - Risk Factors of Incident Kidney Stones in Indian Adults: A Hospital-Based Cross-Sectional Study, Smriti Singh et.al, Cureus, 2023 Feb; 15(2): e35558. Published online 2023 Feb 27. Doi: 10.7759/cureus.35558
View at Publisher | View at Google Scholar - Prevalence and risk factors of kidney stone. Sofia N.H., et.al, GJRA. 2016; 5:183–187. [Google Scholar]
View at Publisher | View at Google Scholar - Epidemiology of stone disease in Northern India; pp. 39–46, Ganesa Moni R., et.al, Urolithiasis. Springer; London, UK: 2012.
View at Publisher | View at Google Scholar - The Demographic Diversity of Food Intake and Prevalence of Kidney Stone Diseases in the Indian Continent, Manalee Guha, et.al, Foods, 2019; 8(1): 37.
View at Publisher | View at Google Scholar - Kidney Stone Prevalence Among Adolescents on the Rise- Amrita Surendranath,
View at Publisher | View at Google Scholar - Kidney Stones and Teens: Causes, Symptoms and Prevention.
View at Publisher | View at Google Scholar - A 13-year hospital-based study on the trend of urinary stone disease in Uttarakhand, India. Kakkar M, Kakkar R. Nepal J Epidemiol. 2021; 11:949-958.
View at Publisher | View at Google Scholar - The demographic diversity of food intake and prevalence of kidney stone diseases in the Indian continent. Guha M, Banerjee et. Al, M. Foods. 2019; 8:37.
View at Publisher | View at Google Scholar - Confounding risk factors and preventative measures driving nephrolithiasis global makeup. Shin S, et.al, World J Nephrol. 2018; 7:129-142.
View at Publisher | View at Google Scholar - The association of increasing BMI and kidney stone disease. Semins MJ, et.al, J Urol. 2010;183:571-575.
View at Publisher | View at Google Scholar - Kidney Stones: Causes, Ayurvedic Treatment & Remedies.
View at Publisher | View at Google Scholar - Best Homeopathic Medicines for Treatment of Chronic Kidney Disease (CKD), Jagat Shah.
View at Publisher | View at Google Scholar
