

Review Article | DOI: https://doi.org/10.31579/2834-796X/082
Giant Left Atrium
President of all nations Morning star hospital, Enayam Thoppu, Kanyakumari District, Tamil nadu state, India.
*Corresponding Author: Ramachandran Muthiah, President of all nations Morning star hospital, Enayam Thoppu, Kanyakumari District, Tamil nadu state, India.
Citation: Ramachandran Muthiah, (2024), Giant Left Atrium, International Journal of Cardiovascular Medicine, 3(6); DOI:10.31579/2834-796X/082
Copyright: © 2024, Ramachandran Muthiah. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 October 2024 | Accepted: 21 October 2024 | Published: 11 November 2024
Keywords: cancer; venous thromboembolism; etiological assessment
Abstract
Aim: To present the aneurysmal dilatation of left atrium due to rheumatic mitral valve disease and its clinical consequences such as arrhythmic, thromboembolic and compressive manifestations.
Introduction: Extreme enlargement of left atrium, usually referred to as giant, gigantic or aneurysmal dilatation is an uncommon finding with a reported incidence of 0.3% in rheumatic heart disease. It is an important clinical risk identifier to predict the outcome of cardiovascular disease.
Case reports: Aneurysmal left atrium correlating with the length of pure mitral regurgitation jet in a 18-year old girl, posterior mitral leaflet prolapse with regurgitation jet swirling around the entire interatrial septum in a 37-year old male, Giant left atrium in mixed mitral valve disease in a 37-year old female and a thrombosed giant left atrium resembling as “coconut” in a 50-year old female were reported.
Conclusion: Giant left atrium may be misinterpreted as right-sided pleural effusion, pericardial effusion and mediastinal tumor on X-ray chest and so echocardiographic evaluation is mandatory to exclude the aneurysmal left atrium in such conditions.
Introduction
The left atrium (LA) is an asymmetrical cavity, often referred as ‘ forgotten chamber’ compared with left ventricle in the past years and it is oriented leftward and posterior to the right atrium in the mediastinum. The walls of the left atrium can be described as superior (roof), posterior (inferoposterior), left lateral, septal, anterior and it is relatively smooth, whereas the appendage is rough with pectinate muscles. The walls are composed of overlapping layers of myocardial fibers with varying thickness, the circular fibers run parallel, the longitudinal fibers perpendicular and the oblique fibers arranged between the two axes to the atrioventricular valve plane [1]. The left atrium functions as a reservoir, conduit, and pump to LV filling. During ventricular systole, the LA receives blood from pulmonary veins as a reservoir (40%), it distends for passive emptying as a conduit (35%) in early diastole, as a pump (25%) [2] by active contraction of atrial muscle in late diastole and mechanically facilitate the transition between the almost continuous flow through the pulmonary venous circulation and intermittent filling of LV. These LA phasic functions depend on LV diastolic properties, the reservoir and pump functions predominate in slow relaxation and the conduit function predominates in restrictive filling phases of cardiac cycle [3].
In normal subjects, the left atrium is an ovoid-elliptical shaped chamber and tends to become more rounded when it is enlarged. LA enlargement is usually induced by pressure and/or volume overload, and various factors and cardiovascular diseases are associated with LA size [4]. The pressure overload is usually secondary to increased LA afterload due to mitral stenosis or LV dysfunction. LA volume overload resulting from mitral regurgitation, arteriovenous fistula, left to right shunt, or high cardiac output state. LA volume has been termed as ‘glycosylated hemoglobin’ of diastolic dysfunction [5] and LA volume index < 29> 39 ml/m2 is severe [7] and > 140 ml/m2 is proposed as ‘giant left atrium’. The normal values of LA size and its enlargement are shown in Table 1.
Left Atrium Size | Women | Men | ||||||
normal | enlarged | normal | enlarged | |||||
mild | moderate | severe | mild | moderate | severe | |||
| Diameter (mm) | 27–38 | 39–42 | 43–46 | ≥47 | 30–40 | 41–46 | 47–52 | ≥52 |
| Volume (ml) | 22–52 | 53–62 | 63–72 | ≥73 | 18–58 | 59–68 | 69–78 | ≥79 |
| Volume/BSA (ml/m²) | 16–28 | 29–33 | 34–39 | ≥40 | 16–28 | 29–33 | 34–39 | ≥40 |
Table 1. Showing the normal values of LA size and its enlargement [8].
LA enlargement is a common feature of rheumatic mitral valve disease. Giant left atrium (size > 6 cm in diameter [9]) is a rare condition associated with rheumatic mitral valve regurgitation or mixed mitral disease with predominant regurgitation, huge thrombus formation [10] and so these cases had been reported.
2.Case Reports
Case 1. PML (posterior mitral leaflet) prolapse causing mitral regurgitation without LA (left atrium) enlargement as shown in Figures 1 and 2 (non-rheumatic) in a 40-year old male. The patient was advised lifelong penicillin prophylaxis and periodic follow up.
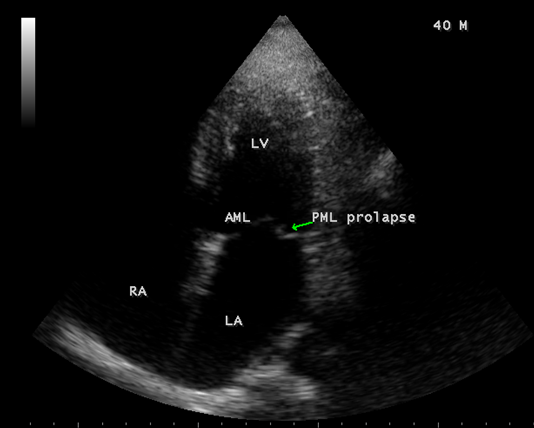
Figure 1. Apical four chamber view showing the PML (posterior mitral leaflet) prolapse (non-rheumatic) in a 40-year-old male. Left atrium (LA) not dilated.
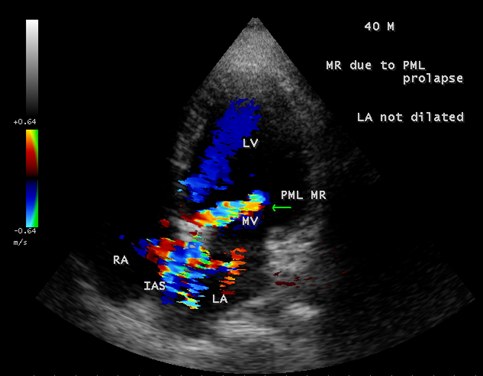
Figure 2. Apical four chamber view showing the mitral regurgitation swirling around IAS (interatrial septum) in a 40-year old male due to PML (posterior mitral leaflet) prolapse. LA (left atrium not dilated)
Case 2. PML (posterior mitral leaflet) prolapse causing severe mitral regurgitation with aneurysmal LA (left atrium) as shown in Figures 3 to 8 due to PML chordal rupture of rheumatic etiology in a 47- year old male. Patient was advised lifelong penicillin prophylaxis and MVR (mitral valve replacement).
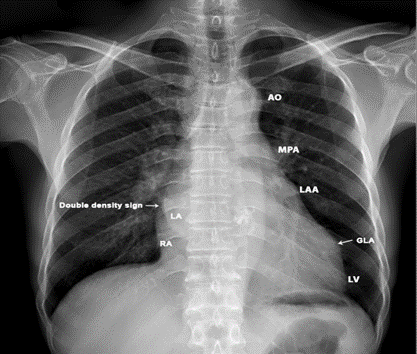
Figure 3. X-ray chest PA (postero-anterior) view showing the “4-bump” left heart border as AO (aortic knuckle), MPA (Main pulmonary artery), LAA (dialed convex left atrial appendage (third mogul sign)), LV (left ventricle). Aneurysmal left atrium elevating the left main stem bronchus which becomes more horizontal and a ‘double density sign in the right heart border (right arrow). Left arrow- showing the GLA (giant left atrium) reaching towards left chest wall.

Figure 4. Parasternal long axis view showing the PML (posterior mitral leaflet) chordal rupture of rheumatic etiology in a 47-year-old male. Both AML (anterior mitral leaflet) and PML (posterior mitral leaflet) of mitral valve are thick and calcified due to rheumatic etiology.
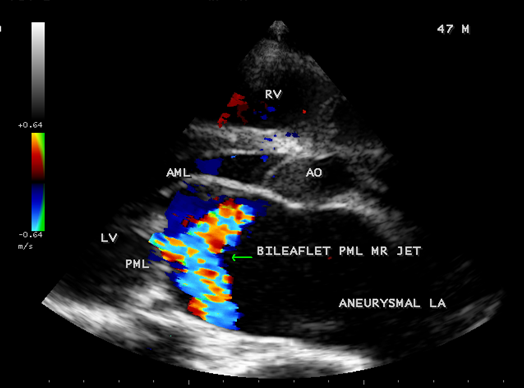
Figure 5. Parasternal long axis view showing the ‘bileaflet’ MR (mitral regurgitation) jet originating from PML (posterior mitral leaflet) in a 47-year-old male.
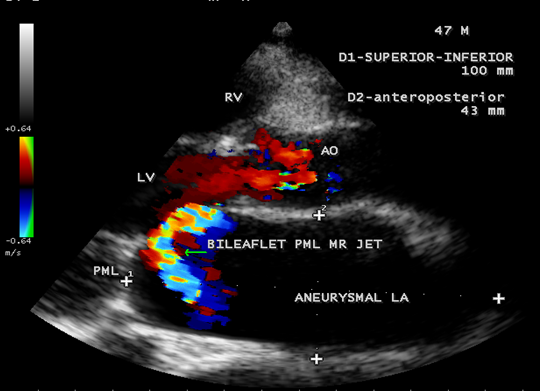
Figure 6. Parasternal long axis view showing the ‘bileaflet’ mitral regurgitation due to PML chordal rupture in a 47- year old male.
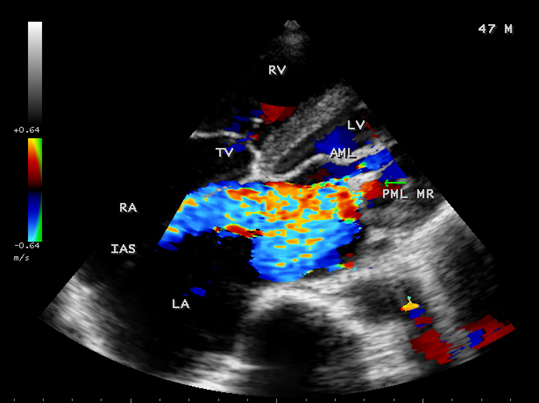
Figure 7. Tilted apical view showing the PML regurgitation in a 47- year old male.
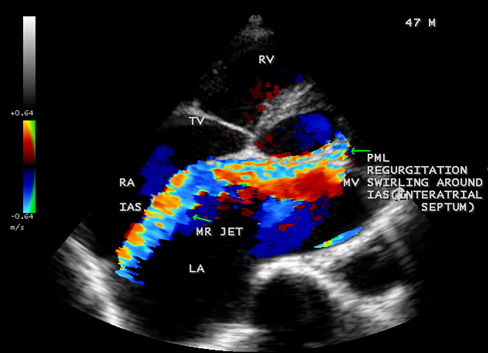
Figure 8. Tilted apical view showing the PML regurgitation swirling around the IAS (interatrial septum) in a 47-year-old male and the left atrium is aneurysmally dilated
Case 3. Aneurysmal left atrium in a 18 –year old girl due to isolated severe rheumatic mitral regurgitation as shown in Figures 9 to 14. The patient was presented with stroke and treated with anticoagulants and antiplatelet agents and, advised lifelong penicillin prophylaxis and MVR (mitral valve replacement).
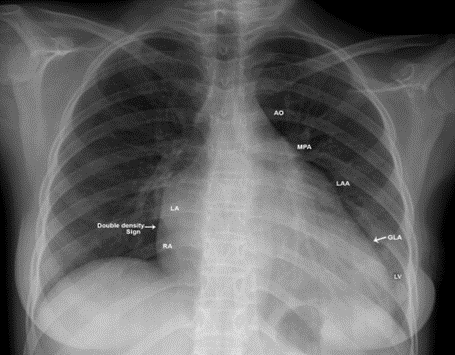
Figure 9. X-ray chest PA (postero-anterior) view showing the dilated LA (left atrium) towards left chest wall in an isolated severe rheumatic mitral regurgitation in a 18-year old girl. The left heart border is ‘4-bump’ as aortic knuckle (AO), MPA (main pulmonary artery), LAA (dilated convex left atrial appendage-third mogul sign) and LV (left ventricle). Right arrow- showing the ‘Double density sign’ of LA enlargement in the right heart border. Left arrow- showing the GLA (giant left atrium) reaching the left chest wall.
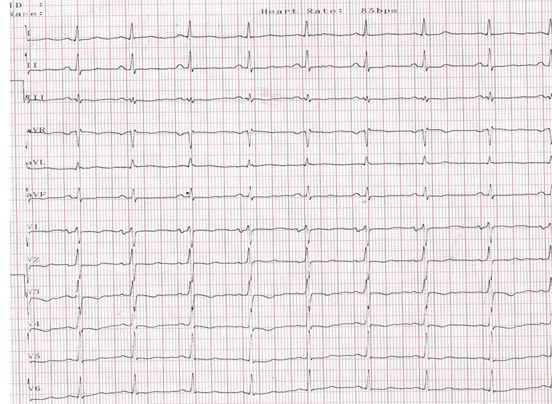
Figure 10. ECG showing LA (left atrial) enlargement as wide P wave (>120 ms) in lead II and increased negative terminal > 0.04 mm in V1. Morris index ( Multiply the length x breadth of the terminal negative portion of the P wave in lead V1 (the P terminal force). This gives the Morris index.
The area exceeds 0.04 mm-sec in left atrial enlargement. (one small square on the ECG taken at 25 mm / s).. Macruz index (widened P width / narrowed PR segment- P/PR segment ≥1.6) IN V1.
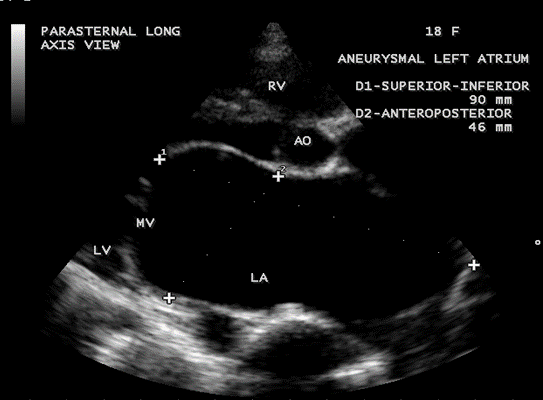
Figure 11. Parasternal long axis view showing the aneurysmal left atrium in a 18-year old girl due to pure rheumatic mitral regurgitation
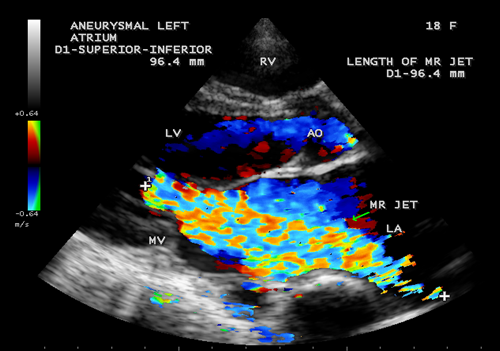
Figure 12. Parasternal long axis view showing the severe mitral regurgitation touching the entire length of dilated left atrium and the length of jet is correlating with superior-inferior dimension of the left atrium in an 18-year-old girl
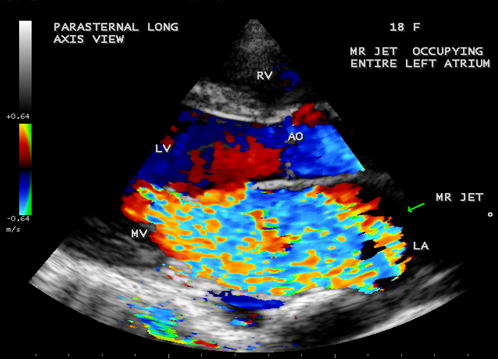
Figure 13. Parasternal long axis view showing the severe rheumatic mitral regurgitation jet occupying the entire aneurysmal left atrium in a 18-year old girl.
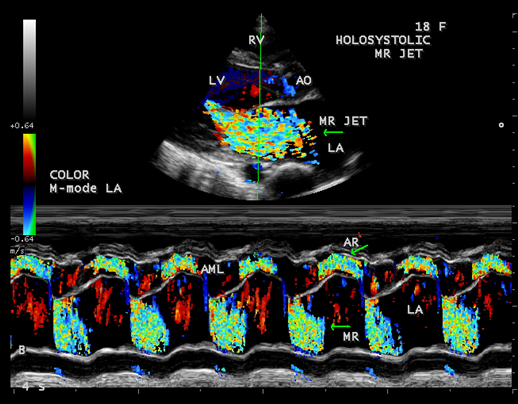
Figure 14. Color-flow M-mode showing the holosystolic mitral regurgitation jet in a 18-year old girl
Case 4. Giant left atrium in mixed rheumatic mitral valve disease- both mitral stenosis and regurgitation as shown in Figures 15 to 20 in a 47-year-old female. The patient was advised lifelong penicillin prophylaxis, MVR (mitral valve replacement), LA volume reduction surgery with Cox-Maze procedure for atrial fibrillation.
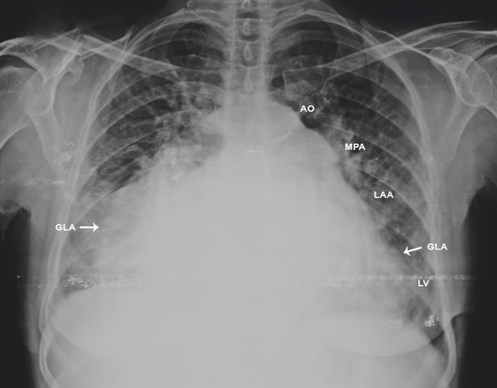
Figure 15. X-ray chest PA (postero-anterior) view---arrows showing the extension of giant left atrium (GLA) to both chest walls.
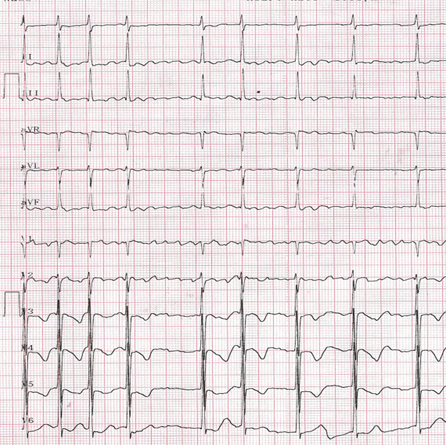
Figure 16. ECG showing the left atrial enlargement, fine atrial fibrillation (fibrillatory waves < 1mm>
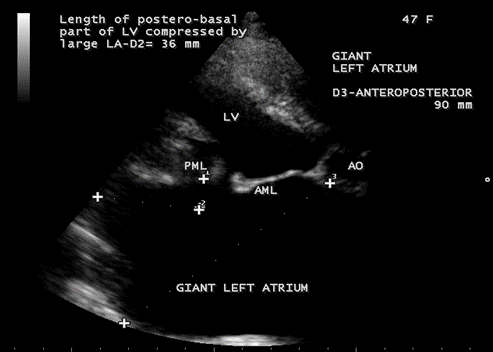
Figure 17. Parasternal long axis view showing the giant left atrium in mixed mitral valve disease in a 47-year-old female. The left atrium is severely enlarged, anatomically distorted and making it difficult to find a correct angle for adequate measurement. The giant left atrium compressing the postero-basal part of LV (left ventricle) and the length of compression is 36 mm.
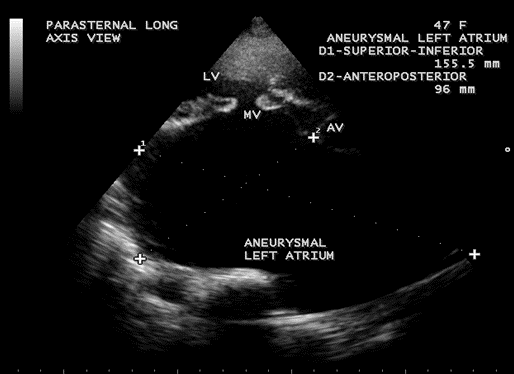
Figure 18. Parasternal long axis view showing the giant left atrium looks like a ‘crown (LV) on a cushion (aneurysmal left atrium)’ appearance in a 47-year-old female.
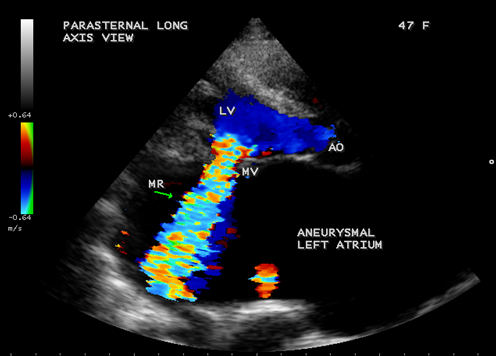
Figure 19. Parasternal long axis view showing the severe mitral regurgitation and giant left atrium in a 47-year-old female.
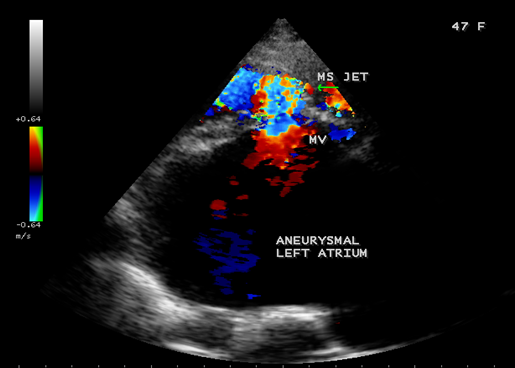
Figure 20. Parasternal long axis view showing the mitral stenosis jet and giant left atrium in a 47-year-old female.
Case 5. Giant left atrium with dense SEC (spontaneous echo contrast) visible as massive thrombus occupying the entire giant left atrium and resembling as “coconut atrium” as shown in Figures 21 to 25 and movie in Figure 26
in rheumatic mitral stenosis in a 50- year old female. Patient was advised lifelong penicillin prophylaxis, Redo MVR (mitral valve replacement) and removal of thrombus with inverted T-shaped biatrial incision (endoatriectomy- transeptal superior approach)
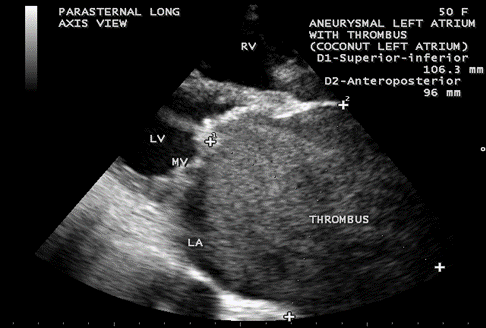
Figure. 21. Parasternal long axis view showing the dense SEC (spontaneous echo contrast) visible as thrombus occupying the entire giant left atrium in a 50-year old female.
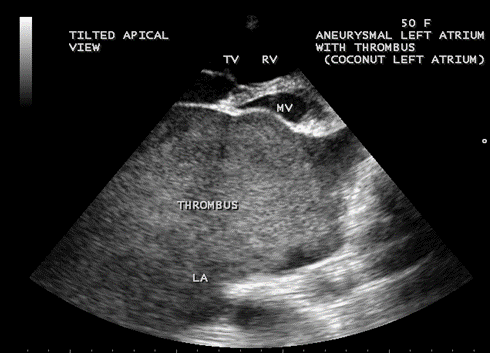
Figure 22. Tilted apical view showing the thrombus occupying the entire Left atrium in a 50-year old female.
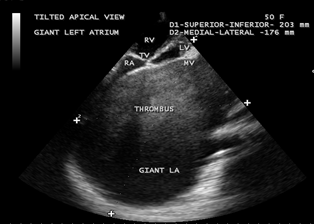
Figure 23. Tilted apical view showing the giant thrombosed left atrium in a 50-year-old female measuring as 203 x 176 mm.

Figure 24. Tilted apical view showing the giant thrombosed left atrium in a 50-year-old female resembling as a “coconut” as in Figure 25
Figure 25. showing the “coconut”.
3.Discussion
Review of literature
In 1849, Hewett was the first to describe the giant left atrium in autopsy series of mitral valve disease [11]. When LA enlarges, it moves rightward and Hurst described the giant left atrium as one that touches the right lateral thoracic wall (giant left atrial syndrome) in chest X-ray and it is almost always caused by rheumatic mitral valve disease [12] with predominant mitral regurgitation than mitral stenosis and atrial fibrillation is mostly present in this condition. In 1984, Piccoli, et al consider giant left atrium when the cardio-thoracic ratio in the chest X-ray is > 0.7 in addition to a left atrial anteroposterior diameter of > 8 cm in transthoracic echocardiography [13]. Massive dilatation of the left atrium occurs in all directions, may reach both chest walls as in Figure 15 and particularly to the right and sometimes to the left as in Figures 3 and 9 [14] Giant LA is rarely observed in non-rheumatic mitral valve involvement and it does not occur in mitral regurgitation due to other causes. Severe mitral regurgitation due to MVP does not produce a giant left atrium since there is no associated primary left atrial disease as shown in Figures 1 and 2. Phua and Brownsberger, et al reported giant left atrium due to mitral valve prolapse [15] and the largest “ non-rheumatic” giant left atrium reported in mitral valve prolapse measured 12 x 13 cm [16]. A giant left atrium associated with PML (posterior mitral leaflet) prolapse) due to severe mitral regurgitation as a result of chordal rupture with rheumatic etiology was shown in Figures 4 to 8. The largest reported giant left atrium due to untreated rheumatic heart disease measured 19.3 x 14.7 cm [17] and 20 x 16.8 cm [18]. Owen, et al misinterpreted a giant left atrium as right-sided pleural effusion and punctured [19], the postmortem examination revealed a severely enlarged left atrium occupying the entire thoracic cavity and this is the first published case of ‘giant left atrium’, a term that was introduced by Fisher, et al [20] in 1956. Schwartzman, et al performed a CT –guided biopsy in a giant left atrium believing it to be a malignant mass [21]. There is no definition of a giant left atrium based on LA volume and an anteroposterior atrial diameter > 65 mm as ‘giant left atrium’, corresponding to 1.6 times the normal value (< 40>Figure 17 and the cut off’s are arbitrary whether an atrium is severely dilated or giant.
Pathogenesis
Left atrial dilatation may be congenital or acquired. The congenital aneurysmal dilatation of left atrium most frequently involves the left atrial appendage, rarely affects the body of left atrium [23] and it may be caused by congenital dysplasia of musculi pectinati and LA muscle bundles related to them [24]. Congenital weakness of the atrium results in local dilation, gradually increases in size and their walls may be composed of hypertrophied myocardium or fibrous tissue [25]. If the aneurysmal wall protruding from the LA has normal myocytes, it is termed as LA diverticulum [26].
Massive enlargement of left atrium is usually associated with an acquired cause of long-standing rheumatic mitral valve disease and its exact etiology is not fully understood. Rheumatic pancarditis damages the entire heart by causing chronic inflammation and weakening its tissues, including the left atrial wall that then dilates more easily. Occasionally, the left atrium can reach extreme sizes even under normal mitral valve function in both adults and children [27]. Histologically, the atrial wall of giant left atrium does not usually reveal Aschoff bodies (perivascular fibrinoid necrosis in the myocardium), the fibrosis and chronic inflammatory changes are mostly present.
In mitral regurgitation, the left atrial size is proportionately related to compliance and the dilated left atrium compensates for increased stress by an initial increase in compliance. This reservoir effect of a large left atrium is beneficial to protect the lungs from pulmonary hypertension and edema [28],[29]. Increased left atrial and pulmonary pressures, in case of very large left atrium ( > 60 mm) provide the substrate as a structural precursor of atrial fibrillation [30],[31] which contributes further atrial dilation in mitral valve disease [32]. The dilated atrium requires more energy to pump blood and lose its elastic properties due to myocarditis, succumbs to deformational change, limiting Laplace’s law application in chronic mitral regurgitation and becomes larger with an increase in LA volume. For an LA diameter of 6 cm, the estimated volume of atrium exceeds 300 ml [33]. The increased LA volume may complicate thrombus formation due to potential stasis with thromboembolic events. The enlarged left atrium may compress the bronchial tree (widening of carinal angle (splaying of carina) > 120 ₀ as shown in Figure 3, stenosis of left main bronchus), left laryngeal nerve (hoarseness due to left vocal cord paralysis- Ortner’s syndrome [34],[35]), inferior and middle lobes of right lung (atelectasis, infection) [36], postero-basal part of left ventricle as in Figure 17 (hemodynamic instability) and esophagus (dysphagia). Isolated LV compression by Giant LA is defined as Type 1 [37], both LV and bronchopulmonary compression is defined as Type II [38] Giant left atrium. Nigri reported a rare complication of giant left atrium, pushing the heart to the right side of the chest and mimicking as dextrocardia [39],[40]. The left atrium extends more to the left side forming the left atrial appendage which becomes convex in the left heart border (third Mogul sign) just below the pulmonary trunk when it is dilated (normally it should be flat or slightly concave) and makes a “4-bump” left heart border as in Figure 3 and 9 that includes the aortic knob, main pulmonary artery, left atrial appendage, and the left border of left ventricle. In mitral stenosis, the body of left atrium is larger than normal and it never produces a giant left atrium, but giant left atrium with rheumatic mitral stenosis was reported [41] and it may be associated with massive thrombus formation as shown in Figures 21 to 24.
Echocardiographic Features
Echocardiography is an excellent, non-invasive technique for obtaining anatomical measurements and it is universally accepted to asses the left atrial size [42], comparable to angiography. Since the left atrium is not a symmetrically shaped 3D structure, the linear dimensions inaccurately represent the LA size, widely used in clinical practice and shown to correlate with angiographic measurements. Expansion of the left atrium in the AP (anteroposterior) dimensions may be constrained by the thoracic cavity between the sternum and the spine. Predominant enlargement in the superior-inferior and medial-lateral dimensions will alter the LA geometry and the AP dimensions also may not be representative of LA size [43]. Kawazoe, et al proposed two echocardiographic criteria to define the giant left atrium [44].
- Large left atrium depicted by M-mode echocardiography with diameter > 65 mm
- Left ventricular posterobasal wall bent inward and lying between the dilated LA cavity and LV cavity. The length of postero-basal part of LV compressed by large LA ≥ 30 mm was defined as ‘ giant left atrium’ [45] as shown in Figure 17.
Cross sectional echocardiography is superior to M-mode echocardiography for measuring left atrial size [46],[47] and it allows the visualization of entire left atrium from different views [48]. The presence and extent of chamber dilatation could not be predicted by the use of a single dimension. In normal subjects, the SI (superior-inferior) dimension being the major axis and the ML (medial-lateral), AP (anteroposterior) dimensions are the minor axes, and the SI dimension is usually the largest among the left atrial diameters and it should include the measurements of all three dimensions to determine the presence and to measure the degree of LA dilatation.
The extreme dilatation of the left atrium is probably related to the jet of regurgitation (or insufficiency), a finding common to all as shown in Figure 12, the jet occupies the entire left atrium as in Figure 13 and a holosystolic pattern in color M-mode echocardiography as shown in Figure 14.
The balloon-like enlargement of the left atrium which occupied the whole of the posterior, right and left mediastinum and the rest of the heart looks like a ‘crown on a cushion’ as shown in Figures 17 and 18 in mixed mitral valve disease (both stenosis and regurgitation) as in Figures 19 and 20.
The LA enlargement was associated with spontaneous echo contrast in the left atrium [49] as shown in Figures 21 to 24. A relationship between LA enlargement and increased risk of stroke was first proposed in 1980’s [50],[51]. LA dilation leads to thinning and fibrosis of myocardial and conducting fibers [52],[53] and thereby results in electrical tissue inhomogeneity, disordered electrical activation and contractility. Every 5 mm increase in LA diameter increases the development of atrial fibrillation by 39% [54] or 4-fold increase in the risk of new AF (atrial fibrillation) with LA diameter > 50 mm [55]. Patients with atrial fibrillation, who usually have LA diameter > 45mm and atrial enlargement may increase refractoriness to medical or electrical conversion of atrial fibrillation [56] into sinus rhythm due to the fibrotic and calcified degeneration of left atrial myocardium. Early cardioversion is avoided in presence of LA thrombus and appropriate anticoagulant therapy is instituted for 6 to 12 weeks and interventional treatments such as PTMC (percutaneous trnsluminal mitral commissurotomy) and CMC (closed mitral commissurotomy) are adopted only after reevaluation by echo. The incidence of LA thrombus among patients with mitral stenosis and atrial fibrillation varies from 7-38 % and it is directly related to the size of left atrium [57], but not all patients with giant left atrium have an associated thrombus formation [58], the thrombus size also varies and this diversity may be due to local factors within the left atrium as shown in Table 2.
Left atrial Endocardial damage Activation of coagulation system within the left atrium High levels of biochemical markers Fibrinopeptide A Thrombin-antithrombin III complex Von Willebrand factor antigen [59],[60]. Paraneoplastic (due to altered intravascular coagulation related to carcinoma breast [61] or lung [62] Rhythm changes (atrial fibrillation or atrial flutter) |
Table 2. Showing the local risk factors for thrombosis within the left atrium
Profuse, dense SEC (spontaneous echo contrast) with its swirling pattern of increased echogenicity and sometimes, it becomes impossible to differentiate dense SEC from the underlying thrombus. A patient with giant left atrium due to rheumatic mitral valve disease with SEC was reported in 2012 [63].
The LA calcification, originally described in 1898 and the first presentation of LA calcification was made by Oppenheimer in 1912 [64]. It is an uncommon complication of long-standing rheumatic valve disease and if heavy calcification was observed in the LA appendage, atrial free wall and the mitral valve apparatus with sparing of interatrial septum, it is termed as ‘porcelain atrium’ [65]. Involvement of dense calcification to the interatrial septum as transmural calcification of entire left atrium is called as ‘coconut atrium’ [66] and calcification of left atrium with pulmonary veins is called as ‘mold-like’ calcification [67]. LA calcification is described as a high-density ring encircling the left atrium on chest-X-ray and Harthome, et al [68] described its appearance as a C-shaped curvilinear density with the opening of the C lying anteriorly in the region of the mitral annulus. This condition is assumed to the end result of extensive rheumatic pancarditis and a classification scheme was proposed for LA calcification [69] as shown in Table 3 and the pathophysiological mechanism of LA calcification was shown in Table 4.
Type A
Type B
Type C | Calcification confined to LA appendage. Mitral stenosis is the underlying lesion often and is almost always associated with thrombus in the appendage
Calcification confined to the free wall of left atrium and mitral valve and is seen in advanced mitral stenosis.
Small area of calcification confined to posterior wall of LA , results from the jet lesion of mitral regurgitation and termed as ‘McCallum’s patch’ |
Table 3. Classification of LA calcification
Previous ulceration of the atrial wall as the origin of calcification A response to the chronic strain forces in the setting of mitral disease Chronic renal failure [70],[71] |
Table 4. Pathophysiological mechanisms for LA calcification
Massive calcification of left atrium, predominantly affects the woman (74%) and it tooks an average duration of 19.7 years (17-20 years) to become manifest in rheumatic mitral stenosis and resembled a coconut shell [72]. The term ‘coconut atrium’ is misnomer to describe this condition and a complete opacification of giant left atrium with dense SEC seen as thrombus as shown in Figure 24, resembling a ‘coconut’ as in Figure 25 and this condition is better termed as ‘coconut atrium’ appropriately.
Management
Medical Therapy
Giant left atrium increases the thromboembolic risk, despite anticoagulant therapy. A Giant left atrium is an indication for the initiation of anticoagulant
therapy and they were anticoagulated with an International Normalized Ratio (INR) ranging between 2.5 and 3.5. Anticoagulants alone seem to be safe approach to reduce thrombosis [73]. However, such medications are not ideal for early use since several days are usually required to achieve the therapeutic INR. The response of an organized thrombus to an anticoagulant therapy may be unpredictable. The thrombus dissolves partially, the shed fragments results in embolization during therapy and the severed thrombus may block the mitral orifice and causes sudden death [74],[75]. Despite anticoagulation with a direct thrombin inhibitor, the oral dabigatran, thrombus occurred in rheumatic mitral stenosis with atrial fibrillation [76]. The non-vitamin K antagonist oral anticoagulants (NOAC)- rivaroxaban are effective alternative to warfarin for resolving thrombus in the left atrium in patients with atrial fibrillation [77] and the reported resolution rate by using vitamin K antagonist is 50-90%. Warfarin is often used for the prevention of thromboembolism in non-valvular atrial fibrillation, and anticoagulation with INR (international normalized ratio) ≥ 2 will reduce the occurrence of ischemic stroke and in-hospital mortality [78].
Thrombolytic therapy is an another option for treating the LA thrombus [79] and shown to be effective in patients with mitral prosthesis with thrombosis [80]. The effectiveness and risk of thrombolytics for an organized or partially organized thrombus or thrombi of long duration is not known clinically. Fragment shedding after resolution and detachment of a large LA thrombus if the stalk was dissolved first could occur after thrombolytic therapy. Before the initiation of thrombolytic therapy, echo characteristics of the thrombus must be carefully analyzed and a fresh, unorganized thrombus appears as homogenous, soft and mobile. A rebound thrombosis after discontinuing anticoagulant therapy was reported by Kadoi,et al [81]. Therefore, maintaining sufficient anticoagulation was crucial following thrombolytic therapy for LA thrombus.
Surgical therapy
The aim of surgery in giant left atrium is to correct the mitral valve abnormalities, to treat compressive manifestations, to prevent thromboembolism and to revert atrial fibrillation into normal sinus rhythm [82].
Mitral valve surgery
Two strategies had been applied as mitral valve surgery alone or mitral valve surgery with LA volume reduction. Some surgeons believe that the effect of rheumatic process on left atrial elastic fibers is irreversible, hence they tend to go only for mitral valve surgery without LA reduction and successful mitral valve surgery alone will result in decrease in LA size, volume and LA pressure.
LA Volume reduction is indicated for the presence of intracardiac or extracardiac compressive symptoms, thrombus with a history of thromboembolic events and prevent recurrent thrombosis by reducing intra-atrial stasis. The volume reduction may be classified into three categories
- Partial plication or resection of inferior atrial wall- the sites of plication include posterior-mitral annulus (para-annular), remaining inferior atrial wall, lateral to the left pulmonary vein and or between right and left pulmonary veins.
A new surgical procedure, para-annular plication of the left atrial wall was attempted to eliminate the compression of basal portion of the posterior wall of the left ventricle to minimize the paradoxical movement and to correct the abnormal direction of the plane of mitral valvular ring
The Mercedes-plasty of the inferior wall- a procedure described by Dzemeshkevich, et al [83], combined GLA (giant left atrium)-plasty with preservation of mitral valve apparatus during MVR (mitral valve replacement) in which the inferior wall of left atrium between the four ostia of pulmonary veins is plicated.
Triangular resection of the inferior wall was described by Sinatra, et al [84] with an advantage to interrupt the wavelets circuits around the pulmonary veins as a beneficial effect of inhibiting the propagation of atrial fibrillation foci.
- Partial plIcation or resection of both inferior and superior atrial walls [85].
Spiral resection of left atrial wall was introduced by Sugiki, et all in 2006 [86]
- Partial heart auto-transplantation [87].
The co-existence of giant left atrium with mitral valve disease provide a significant risk factor in mitral valve surgery and surgical mortality ranging from 8%-23%. The increased operative mortality is proportionately related to high pulmonary systolic pressure, but the intended benefits of reducing a giant left atrium include the elimination of symptoms and alleviating the pressure effects to the left ventricle, bronchus, lung parenchyma and reduction of early postoperative complications related to low cardiac output syndrome and respiratory complications. The simplest modality for size reduction is plIcation of inferior left atrial wall, but the plication of superior wall carries a high risk of bleeding and AV (atrio-ventricular) node blockade.
The plIcation may not necessary when the left atrial diameter is < 80>
Cox-Maze procedure is a viable option to treat long-standing persistent atrial fibrillation in patients with giant left atrium. The aim of the procedure is to divide the macro-reentry circuits and to direct the electrical waves from the sinoatrial node to the atria and atrio-ventricular node. During the procedure, a number of incisions are made on the left and right atrium to form scar tissue, which does not conduct electricity and disrupts the path of abnormal electrical impulses. The scar tissue also prevents erratic electrical signals from recurring. After the incisions are made, the atrium is sewn together to allow it to hold blood and contract to push blood into the ventricle.. Normal sinus rhythm had been reported to range from 67% to 98% [89] and the efficacy of Maze procedure in restoration of atrial contraction in giant left atrium and in those without it are compared after one year follow-up as normal sinus rhythm in ECG was 53% and 75%, regaining atrial contraction as appearance of A wave in pulsed Doppler with a peak velocity of at least 0.10 m/s was 20% and 50% respectively. The bigger the left atrium, the lower is the percent of restoration of sinus rhythm. More than 90% of patients with a preoperative LA size < 57> 85 mm, the success rate was 0 % [92].
Scherer, et al showed that LA volume reduction concomitant with mitral valve surgery restored postoperative sinus rhythm [93], but postoperative LA diameter was significantly smaller in patients who attained sinus rhythm by radiofrequency (RF) Maze procedure. Mitral valve surgery alone may not reduce the enlarged LA size and direct surgical management of giant left atrium will reduce the LA size, and the restoration of sinus rhythm in atrial size reduction was 77.3% whereas without reduction, it is only 61.1%.
If the thrombus is organized, surgery is indicated and surgical intervention may be a conservative modality in very large acute LA thrombus. Removal of an organized thrombus from the left atrium can be challenging especially when it is huge in size. The presence of dense adhesions and absence of cleavage plane make its removal difficult. Thrombectomy can be performed by an inverted T-shaped biatrial incision and the whole thrombus was completely removed intact. Under these circumstances, the residual organized material can be left. Lim and Colleagues suggested the use of autologous pericardial patch to cover these areas to avoid future thrombus formation [94].
Calcification of left atrial wall constitute a major complication and risk to mitral valve surgery due to difficulty in entering the left atrium. Massive calcification of LA wall can cause recurrent thrombosis despite the therapeutic anticoagulant level following a surgical thrombectomy [95]. LA calcification was progressed after mitral valve replacement despite there was no definite LA wall calcification at the time of surgery and it was due to previously formed rheumatic ulceration of the atrial wall as the origin of calcification and its progression.
Roberts et al {96} reported that calcific deposits prevented the left atrium from dilating, decreased its compliance , and caused the elevated LA pressure to be transmitted to the pulmonary vessels and the right ventricle, leading to tricuspid insufficiency. Thus, if a patient who had rheumatic heart disease and underwent mitral valve replacement, suffer right heart failure, extensive LA calcification should be considered.
Surgery should be considered as one option of the treatment for atrial calcification [97]. The accepted surgical treatment of LA calcification is a total endoatriectomy with mitral valve replacement. The interatrial septum serves as the surgical cleavage plane, since this area is noncalcified and is therefore exploited in order to prevent embolization and hemorrhage when a thrombus is present, but it is difficult to suture the calcified structures. The presence of coconut atrium (calcified interatrial wall) will significantly complicate surgery and ncreases the mortality. Mitral annular calcification may progress to liquefaction necrosis, referred to as “caseous necrosis” which can make mitral valve surgery very difficult [98]. Calcification of interatrial septum and caseous necrosis of mitral annulus could be potential contraindications to mitral valve surgery. Dense calcification of atrial wall can prevent visualization of the interior of the chamber so that intracavitary thrombus and the septum cannot be seen [99]. If there is evidence of complete transmural calcification, ie, septum cannot be visualized by TEE (transesophageal echocardiography) and appears to be calcific by CT (computed tomography), suspect “coconut atrium” and it is impossible to incise. In such cases, the calcified endothelium on the atrial septum and the free wall of the left atrium was pealed off (endoatriectomy) and the rim of interatrial wall was reconstructed and closed with a bovine pericardium. Redo MVR was performed with endoatriectomy upon transeptal superior approach [100].
Outcome
A report of De Sanctis, who consider patients with GLA (giant left atrium) to have a relatively benign course even when not operated upon [101] and in rare cases, the patients may remain asymptomatic. No attempt was made to diminish the size of the left atrium by plication or excision as advocated by Johnson [102] or Le Roux [103]. There does not seem to be sufficient evidence that this procedure is of benefit. Morbidity of GLA comes from compression of intracardiac and adjacent extracardiac structures. Tamura et al {104} presented a case of severe mitral stenosis and regurgitation, undergone mitral valve replacement with left atrial volume reduction and showed relief of compression, improvement in respiratory function with a decrease in carinal angle in the immediate postoperative period.
The coexistence of giant left atrium significantly increases the operative mortality from 7% to 20% in mitral valve surgery. Surgical resection is the treatment of choice, even in asymptomatic patients, because of the risk of rupture, systemic embolism, heart failure, arrhythmias or extrinsic compression of trachea or esophagus [105] and the surgeons should consider the risks and beneficial effects of various surgical options when managing the patients with GLA (giant left atrium).
4.Conclusion
Long-standing mitral valve disease is associated with enlargement of left atrium as a compensatory mechanism with a reported incidence of 19%. Giant left atrium is seen in only 3-4% of patients and such a low incidence is probably related to an early development of pulmonary hypertension, its subsequent effect on right ventricular output and the pressure and volume overload in the left atrium are reduced. A giant thrombosed left atrium resembling as a “coconut”, the largest one reported in the literature was found by 2D Transthoracic echocardiography at this hospital in India.
References
- McAlpine,W.,A.,(1975) Heart And Coronary Arteries: An Anatomical Atlas For Clinical Diagnosis, Radiological Investigation, And Surgical Treatment, Springer, Berlin, Germany.
View at Publisher | View at Google Scholar - Lang,R.,M.,Bierig,M.,Devereux,R.,B., et al (2005) ”Recommendations For Chamber Quantification: A Report From The American Society Echocardiography’s Guidelines And Standard Committee And The Chamber Quantification Writing Group, Developed In Conjunction With The European Association of Echocardiography, A Branch of The European Society of Cardiology”, Journal of The American Society of Echocardiography, Volume 18, No 12, PP 1440-1463.
View at Publisher | View at Google Scholar - Prioli,A., Marino,P., Lanzoni,L.,Zardini,P.,(1998) Increasing Degrees of Left Ventricular Filling Impairment Modulate Left Atrial Function In Humans, American Journal of Cardiology, 82(6), 756-761.
View at Publisher | View at Google Scholar - Abhayaratna,W.,P.,Seward,J.,B.,Appleton,C.,P.,Douglas,P.,S.,Oh,J.,K.,Tajik, A.,J.,Tsang,T.,S.,(2006) Left Atrial Size : Physiologic Determinants And Clinical Applications, Journal of American College of Cardiology, 47, 2357-2363.
View at Publisher | View at Google Scholar - Alingandula,A., et al (2016) Detection of Left Atrial Enlargement by Echocardiography And Electrocardiogram, International Journal of Scientific Study, 4 (5), 1-5.
View at Publisher | View at Google Scholar - Paulus,W.,J., Tschope, C., Sanderson, J.,E.,et al (2007)How to Diagnose Diastolic Heart Function: A Consensus Statement on The Diagnosis of Heart Failure With Normal Left Ventricular Ejection Fraction by The Heart Failure And Echocardiography Association of The European Society of Cardiology, European Heart Journal, 28(20), 2539-2550.
View at Publisher | View at Google Scholar - Tsang,T.,S., Abhayaratna,W.,P., Barnes, M.,E.,et al (2006) “ Predicton of Cardiovascular Outcomes With Left Atrial Size: Is Volume Superior to Area Diameter”, Journal of The American College of Cardiology, 47 (5), 1018-1023.
View at Publisher | View at Google Scholar - Lang, R,.M., Bierig, M., Devereux, R.,B., Flachskampf, F.,A., Foster, E., Pellikka, P.,A., Picard, M.,H., Roman, M.,J., Seward, J, Shanewise, J, Solomon, S., Spencer, K.,T., St John Sutton, M., Stewart, W., (2006).
View at Publisher | View at Google Scholar - Isomura,T.,Hisatomi,K.,Hirano,A.,(1993)Left Atrial Plication: Journal of Cardiac Surgery, 8, 365-370.
View at Publisher | View at Google Scholar - Ahmad,K., Darwazah, Hamdy El Sayed (2013) Giant Left Atrium Associated With Massive Thrombus Formation, Thrombosis Journal, 11 (1), 5
View at Publisher | View at Google Scholar - Hewett,P.,(1849) Aneurysmal Dilatation of Left Auricle With Thickening And Contraction of Left Auriculoventricular Opening, Transactions of the Pathological Society of London; 1850:2-193.
View at Publisher | View at Google Scholar - Hurst, J.,W.,(2001) Memories of Patients With A Giant Left Atrium, Circulation, 104, 2630-2631.
View at Publisher | View at Google Scholar - Piccoli,G.,P.,Massini,C., Di Eusanio, G., et al (1984) Giant Left Atrium And Mitral Valve Disease: Early And Late Results of Surgical Treatment In 40 Cases, Journal of Cardiovascular Surgery (Torino), 25, 328-336.
View at Publisher | View at Google Scholar - Plaschkes,J, Borman,J,B., Merin,G., Milwidsky,H.,(1971) Giant Left Atrium In Rheumatic Heart Disease, A Report of 18 Cases Treated By Mitral Valve Replacement , Annals of Surgery, 174, 194-201, Figures 1 ton 4 and 5(a).
View at Publisher | View at Google Scholar - Brownsberger,R.,J., Morrelli,H.,F., (1988) Hoarseness Due to Mitral Valve Prolapse, Journal of the American Geriatrics Society, 36, 442-443.
View at Publisher | View at Google Scholar - Imran Ahmed, Achycet Sarkar, Arindam Pande, Chanchal Kundu (2015) A “Non-Rheumatic“ Giant Left Atrium, Annals of Pediatric Cardiology,8(1), 95-97.
View at Publisher | View at Google Scholar - Ozkan,A.,Tuncer,A., Ozkan,M.,(2012) Giant Left Atrium, Journal of The American College of Cardiology, 60,e13 (8).705-790
View at Publisher | View at Google Scholar - Merwaha, et al (2017) Extent of Left Atrial Enlargement In Rheumatic Mitral Valve Disease, Journal of Cardiovascular Disease & Diagnosis, 5,2.
View at Publisher | View at Google Scholar - Owen,I.,Fenton,W.,J.,(1901) A Case of Extreme Dilatation of The Left Auricle of The Heart, Transactions of the Clinical Society of London, 34, 183-191.
View at Publisher | View at Google Scholar - Fisher,D.,L.,Ford,W.,B.,Kent,E.,M.,Neville,J.,F.,(1956) Mitral Valve Surgery And Left Heart Catheterization In Giant Left Atrium, American Medical Association, Archives of Surgery, 73, 503-507.
View at Publisher | View at Google Scholar - Schwartzman,P.,R., White,R.,D.,(2001) Giant Left Atrium, Circulation, 104, e 28-29.
View at Publisher | View at Google Scholar - Tardu Ozkartal, Felix C Tanner, Markus Niemann (2010) Asymptomatic Post- Rheumatic Giant Left Atrium, World Journal of Cardiology, 8(6), 375-378.
View at Publisher | View at Google Scholar - Foale,R.,A., Gibson,T.,C.,Guyer,D.,E.,Gillam,I.,King,M.,E.,Weyman,A.,F.,(1982) Congenital Aneurysms of The Left Atrium: Recognition By Cross-Sectional Echocardiography, Circulation, 66, 1065-1069.
View at Publisher | View at Google Scholar - Yao,R., Hunsaker,R.,P.,Gelman, B., (2008) An Unusual Echocardiogram, Journal of Cardiothoracic And Vascular Anesthesia, 22, 636-638.
View at Publisher | View at Google Scholar - Terada,H.,Tanaka,Y., Kashima,K.,Sannou,K.,Arima,T.,(2000) Left Atrial Diverticulum Associated With Severe Mitral Regurgitation, Japanese Circulation Journal, 64, 474-476.
View at Publisher | View at Google Scholar - Nagai,T.,Fujii,A.,Nishimura,K.,Inoue,K.,Suzuki,J.,Kido,T.,Nakamura,M.,Matsumoto,Y.,Izutani,H., Mochizuki,T.,Kawachi,K., Higaki,J.,Ogimoto,A.,(2011) A Large Thrombus Originating From Left Atrial Diverticulum: A New Concern For Catheter Ablation of Atrial Fibrillation, Circulation, 124, 1086-1088.
View at Publisher | View at Google Scholar - Ates,M.,Sensoz,Y.,Abay,G.,Akcar,M.,(2006)Giant Left Atrium With Rheumatic Mitral Stenosis, Texas Heart Institute Journal, 33, 389-391.
View at Publisher | View at Google Scholar - Schwammenthal,E., Vered,Z., Agranat,O., Kaplinsky,E., Rabinowitz,B., Feinberg,M.,S., (2000) Impact of Atrioventricular Compliance On Pulmonary Artery Pressure In Mitral Stenosis: An Exercise Echocardiographic Study, Circulation, 102, 2378-2384.
View at Publisher | View at Google Scholar - Grimes,R.,V., Levine,R.,A., Walker,P.,G., Yoganathan,A.,P.,(1995) Dynamics of Systolic Pulmonary Venous Flow In Mitral Regurgitation: Mathematical Modelling of The Pulmonary Venous System And Atrium, Journal of The American Society of Echocardiography, 8, 631-642.
View at Publisher | View at Google Scholar - Kopecky,S., Gersh,B., McGoon,M., Whisnant,J,P., Holmes,D.,R., Jr, Ilstrup,D.,M., Frye,R.,L.,(1987) The Natural History of Lone Atrial Fibrillation: A Population Based Study Over Three Decades, New England Journal of Medicine, 317, 669-674.
View at Publisher | View at Google Scholar - Henry,W.,L., Morganroth,J, Pearlman,A., Clark,C.,E., Redwood,D.,R., Itscoitz, S.,B., Epstein,S.,E., (1976) Relation Between Echocardiographically Determined Left Atrial Size And Atrial Fibrillation, Circulation, 53,2, 273-279.
View at Publisher | View at Google Scholar - Sanfalippo,A., Abascal,V., Sheehan,M., Oertel,L.,B., Harrigan,P., Hughes,R.,A., Weyman,A.,E., (1990) Atrial Enlargement As A Consequence of Atrial Fibrillation, Circulation, 82, 792-797.
View at Publisher | View at Google Scholar - Matsuda, H., Nakao,M., Nohara,H., Higami,T., Mukohara,N., Asada,T., Ogama,K., Kawamura,T.,,(1990) The Causes of Prolonged Postoperative Respiratory Care In Mitral Valve Disease With A Giant Left Atrium, Japanese Journal of Thoracic Surgery, 43, 172-182.
View at Publisher | View at Google Scholar - Morgan,A., Mourant,A.,(1980) Left Vocal Cord Paralysis And Dysphagia In Mitral Valve Disease, British Heart Journal, 43, 470-473.
View at Publisher | View at Google Scholar - Ortner, N.,(1897) Recurrent Laryngeal Nerve Paralysis From Mitral Stenosis, Wiener Klinische Wochenschrift, 33, 753-755.
View at Publisher | View at Google Scholar - Phua,G.,Eng,P.,Lim,S.,(2005) Beyond Ortner’s Syndrome – Unusual Pulmonary Complications of The Giant Left Atrium, Annals of The Academy of Medicine, Singapore, 34, 642-645
View at Publisher | View at Google Scholar - Kothari, A., Kothari, K.,(2005) A Giant Left Atrium, Journal of Postgraduate Medicine , 51, 49-50.
View at Publisher | View at Google Scholar - Kawazoe,K., Beppu,S., Takahara,Y., Nakajima,N., Tanaka,K., Ichihashi,K., Fujita,T., Manabe,H., (1983) Surgical Treatment of Giant Left Atrium Combined With Mitral Valve Disease, Plication Procedure For Reduction of Compression to The Left Ventricle, Bronchus, And Pulmonary Parenchyma, The Journal of Thoracic And Cardiovascular Surgery, 85, 885-892.
View at Publisher | View at Google Scholar - Nigri,M.,Fernandes,J,L., Rochittee, C.,E., (2007) Giant Left Atrium And A Right Sided Heart, Heart, 93, 475.
View at Publisher | View at Google Scholar - Michael Funk, Margarita Perez, Orlando Santana (2010) Asymptomatic Giant Left Atrium, Clinical Cardiology, 33,6, E 104- E 105, Figure 1.
View at Publisher | View at Google Scholar - Mehmet Ates, Yawz Sensoz, Gunseli Abay, Murat Akcar (2006) Giant Left Atrium With Rheumatic Mitral Stenosis, Texas Heart Institute Journal, 33 (3), 389-391.
View at Publisher | View at Google Scholar - Hirata, T.,Wolfe, S.,B., Popp,R.,L.,Helman, C.,H., Feigenbaum,H.,(1969) Estimation of Left Atrial Size Using Ultrasound, American Heart Journal, 78, 43-52.
View at Publisher | View at Google Scholar - Lemire, F., Tajik,A.,J, Hagler, D.,J, (1976) “Asymmetric Left Atrial Enlargement: An Echocardiographic Observation”, Chest, 69, 6, 779-781.
View at Publisher | View at Google Scholar - Anandan,P.,K.,Shukkarbhai,P.,J., Cholenahally,M.,N.,(2017) Giant Left And Right Atrium In Rheumatic Mitral Stenosis And Regurgitation, Journal of Cardiovascular Echography, 25, 113-115.
View at Publisher | View at Google Scholar - Fujita, T., et al (1982) Surgical Treatment On Mitral Valvular Disease And Giant Left Atrium- The Effect of Para-Annular Plication On Left Atrium, Japanese Circulation Journal, 46, 42-426.
View at Publisher | View at Google Scholar - Feigenbaum,H.,(1981) Echocardiography, 3rd Edition, Philadelphia: Lea & Febiger, 168-176
View at Publisher | View at Google Scholar - Schabelman,S.,E., Schiller,N.,B.,Silverman, N.,H.,Ports,T.,A.,(1981) Left Atrial Volume Estimation By Two-Dimensional Echocardiography, Catheterization And Cardiovascular Diagnosis, 7, 165-178.
View at Publisher | View at Google Scholar - Weyman,A.,E.,(1982) Cross-Sectional Echocardiography, Philadelphia: Lee & Febiger, 192-198, 498-501
View at Publisher | View at Google Scholar - Providencia,R., et al (2012) Possible Refinement of Clinical Thromboembolism Assessment In Patients With Atrial Fibrillation Using Echocardiographic Parameters, Europace, I, 36-45.
View at Publisher | View at Google Scholar - Caplan,L.,R., D’Cruz,I., Hier,D.,B.,Reddy,H., Shah,S., (1986)Atrial Size, Atrial Fibrillation, And Stroke, Annals of Neurology, 19, 158-161.
View at Publisher | View at Google Scholar - Aronow, W.,S.,Gutstein,H., Hsieh,F.,Y.,(1989) Risk Factors For Thromboembolic Stroke In Elderly Patients With Chronic Atrial Fibrillation, American Journal of Cardiology, 63, 366-367.
View at Publisher | View at Google Scholar - Davies,M.,J, Pomerance,A.,(1972) Pathology of Atrial Fibrillation In Man, British Heart Journal, 34, 520-525.
View at Publisher | View at Google Scholar - Bailey,G.,W.,H.,Braniff,B.,A.,Hancock,E.,W.,Cohn,K.,E.,(1968)Relation of Left Atrial Pathology To Atrial Fibrillation In Mitral Valvular Disease, Annals of Internal Medicine, 69, 13-20
View at Publisher | View at Google Scholar - Vazini,S.,M., Larson, M.,G.,Benjamin,E.,J, Levy,D.,(1994)Echocardiographic Prediction of Nonrheumatic Atrial Fibrillation, The Framingham Heart Study, Circulation, 96(7), 2455-2461
View at Publisher | View at Google Scholar - Psaty, B.,M.,Manolio, T.,A., Kuller, L.,H.,et al (1997) Incidence of And Risk Factors For Atrial Fibrillation In Older Adults, Circulation, 96(7), 2455-2461
View at Publisher | View at Google Scholar - Hoglund,C., Rosenhamer,G.,(1985) Echocardiographic Left Atrial Dimension As A Predictor of Maintaining Sinus Rhythm After Conversion of Atrial Fibrillation, Acta Medica Scandinavica, 217, 411-415.
View at Publisher | View at Google Scholar - Farman,M.,T.,Sial, J.,A., Khan,N., Rahu, Q.,A., Tasneem,H., Ishaq,H., (2010)Severe Mitral Stenosis With Atrial Fibrillation, A Harbinger of Thromboembolism, Journal of Pakistan Medical Association, 60 (6), 439-443.
View at Publisher | View at Google Scholar - Yazici, H.,U., Akcay,B., Ozturk,U., Tassal,A., (2010) A Giant Left Atrium, Turk Kardiyologi Dernegi Arsivi, 38, 223.
View at Publisher | View at Google Scholar - Goldsmith, I., Kumar,P., Carter,P., Blann,A.,D., Patel,R.,L., Lip,G.,Y.,(2000) Atrial Endocardial Changes In Mitral Valve Disease, A Scanning Electron Microscopy Study, American Heart Journal, 140 (5), 777-784
View at Publisher | View at Google Scholar - Yamamoto,K.,Ikeda,U.,Seino,Y.,Mito,H.,Fujikawa,H.,Sekiguchi,H.,Shimada,K.,(1995) Coagulation Activity Is Increased In The Left Atrium of Patients With Mitral Stenosis, Journal of American College of Cardiology, 25(1), 107-112.
View at Publisher | View at Google Scholar - Wrisley,D., Giambartolomel,A., Lee,I.,Brownlee,W.(1989)Massive Left Atrial Thrombus: A Possible Paraneoplastic Complication of Breast Carcinoma, Clinical Cardiology, 12, 607-608
View at Publisher | View at Google Scholar - Dong Xie, Jiaan Ding, Xiano Zhou, Chang Chen, Deping Zhao, Gening Jiang (2015) Tumor Thrombus In Left Atrium From Pulmonary Adenosquamous Carcinoma, Asian Cardiovascular And Thoracic Annals, 23(1), 75-77.
View at Publisher | View at Google Scholar - Ahmet Coskun Ozdemir, Bilgin Emrecan (2012) Simple Left Atrial Reduction In Giant Left Atrium Accompanying Mitral Stenosis, Kardiochirurgia i Torakochirurgia Polska, 9(4), 474-476, Figure I (A).
View at Publisher | View at Google Scholar - Oppenheimer,B.,S.,(1912) Calcification And Osteogenic Change of The Left Auricle In A Case of Auricular Fibrillation, Proceedings of The New York Pathological Society ,12, 213-215.
View at Publisher | View at Google Scholar - Leacock,K., Duerinckx, A.,J., Davis,B., (2011) Porcelain Atrium: A Case Report With Literature Review, Case Reports in Radiology, 501396.
View at Publisher | View at Google Scholar - Del Campo,C., Weinstein,P., Kunnelis,C., Di Stefano,P.,Ebers,G.,M.,(2000) Coconut Atrium: Transmural Calcification of The Entire Left Atrium, Texas Heart Institute Journal, 27, 49-51.
View at Publisher | View at Google Scholar - Ruvolo,G., Greco,E.,Speziale,G., Mercogliano,D., Marino,B., (1994) “ Mold-Like” Calcification of The Left Atrium And of The Pulmonary Veins, Total Endoatriectomy In A Patient Undergoing Mitral Valve Replacement, European Journal of Cardio-Thoracic Surgery, 8, 54-55.
View at Publisher | View at Google Scholar - Harthorne,W., Seltzer,R.,A., Austen,W.,G.,(1966) “Left Atrial Calcification: Review of Literature And Proposed Management”, Circulation, 3(2), 198-210.
View at Publisher | View at Google Scholar - Shaw,D.,R.,Chen,T.,T.,Lester,R.,G., (1976) “X-Ray Appearance And Clinical Significance of Left Atrial Wall Calcification” Investigative Radiology, 11 (6), 501-507.
View at Publisher | View at Google Scholar - Koroglu,M.,Chen,P.,S.,Oto,A.,Koroglu,B.,K.,(2005) Left Atrial, Pulmonary Vein And Dural Calcification In A Patient With Arrhythmia And Chronic Renal Failure, JBR-BTR (Journal Belge de Radiologie - Belgisch Tijdschrift voor Radiologi) 88, 78-79.
View at Publisher | View at Google Scholar - Lahey,T., Horton,S., (2002) Massive Left Atrial Calcification And Devastating Systemic Emboli In A Patient With Chronic Renal Failure, American Journal of Kidney Diseases, 40, 416-419.
View at Publisher | View at Google Scholar - George Pulikal, Andrew Marshall (2006) Complete Calcification of A Rheumatic Left Atrium, New England Journal of Medicine, 354, 2262, Figures (b), (e), (f)
View at Publisher | View at Google Scholar - Ageno,W., Turpie,A.,G., Steidl,L.,Ambrosini,F., Cattaneo,R., Codari,R.,L.,Nardo, B., Venco,A., (2001) Comparision of A Daily Fixed 2.5 mg Warfarin Dose With A 5 mg, International Normalized Ratio Adjusted, Warfarin Dose Initially Following Heart Valve Replacement, American Journal of Cardiology, 88,40-44.
View at Publisher | View at Google Scholar - Iga,K.,Izumi,C., Konishi,T.,(1999) Formation of A Left Atrial Ball Thrombus From A Large Mural Thrombus 4 Days After An Embolic Episode, International Journal of Cardiology, 70, 83-86.
View at Publisher | View at Google Scholar - Fraser,A.,G., Angelini,G.,D., Ikram,S., Butchart, E.,G., (1988)Left Atrial Ball Thrombus: Echocardiographic Feature And Clinical Implications, European Heart Journal, 9, 672-677.
View at Publisher | View at Google Scholar - Sushil Allen Luis, Karl Poon, Chris Luis, Akhil Shukla, Nicholas Bett, Christian Hamilton-Craig (2013) Massive Left Atrial Thrombus In A Patient With Rheumatic Mitral Stenosis And Atrial Fibrillation While Anticoagulated With Dabigatran, Circulation: Cardiovascular Imaging, 6, 491-492.
View at Publisher | View at Google Scholar - Todd Neale (2016) Rivaroxaban May Help Dissolve Left Atrial Thrombus In Patients With Atrial Fibrillation, tctMD, The Heart Beat
View at Publisher | View at Google Scholar - Hylek,E.,M.,Go,A.,S.,Chang,Y., Jenvold,N.,G.,Henault,L.,E.,Selby,J.,V.,et al (2003) Effect of Intensity of Oral Anticoagulation On Stroke Severity And Mortality In Atrial Fibrillation, New England Journal of Medicine, 349, 1019-1026.
View at Publisher | View at Google Scholar - Hassan,W., El Shaer,F., Fawzy, M.,E., Akhras,N., Abdullah,R., Fadel,B.,M.(2004) Successful Lysis of Intra-cardiac Thrombi With Steptokinase In Patients With Renal Failure, Two Case Reports And Review of The Literature, Journal of Thrombosis And Thrombolysis, 18, 145-149.
View at Publisher | View at Google Scholar - Gupta,D., Kothari, S.,S., Batil, V.,K.,Goswami,K.,C., Talwar,K.,K.,Man Chanda, S.,C., et al (2000) Thrombolytic Therapy For Prosthetic Valve Thrombosis, Short-And Long – Term Results, American Heart Journal, 140, 906-916
View at Publisher | View at Google Scholar - Kadoi,Y.,Sakaguchi,M.,Tatahashi,K.,Saito,S.,Goto, F.,(2004) Acute Thrombus Formation In The Left Atrium After The Termination of Warfarin, Journal of Anesthesia, 18, 224-227.
View at Publisher | View at Google Scholar - Apostolakis,E., Shuhaiber,J.,H.(2008) The Surgical Management of Giant Left Atrium, European Journal of Cardiothoracic Surgery, 33, 182-190.
View at Publisher | View at Google Scholar - Dzemeshkevich,S.,Korolev,S.,Frolova,J,Skridlevskaya,E.,Margolina,A.,Podlesskich,Y.,Sinitsin,V.,Akchurin,R.,(2001)Isolated Replacement of The Mitral Leaflets And ‘Mercedes-Plastics of The Giant Left Atrium: Surgery For Patients With Left Ventricle Dysfunction And Left Atrium Enlargement, Journal of Cardiovascular Surgery (Torino), 42, 505-508.
View at Publisher | View at Google Scholar - Sinatra,R., Pulitani,I.,Antonazzo,A., Melina,G.,(2001) A Novel Technique For Giant Left Atrium Reduction: European Journal of Cardiothoracic Surgery, 20, 412-414.
View at Publisher | View at Google Scholar - Yuasa,S., Soeda, T., Masuyama,S., Shimizu,K., Matsuda,M.,(2003) Surgical Treatment of Giant Left Atrium Using A Combined Superior-Transeptal Approach, Annals of Thoracic Surgery, 75, 1985-1986.
View at Publisher | View at Google Scholar - Sugiki,H., Murashita,T., Yasuda,K.,Doi, H.(2006)Novel Technique For Volume Reduction of Giant Left Atrium: Simple And Effective ‘Spiral Resection’ Method, Annals of Thoracic Surgery, 81, 378-380.
View at Publisher | View at Google Scholar - Lessana,A., Scorsin,M.,Scheuble,C., Raffoul,R., Rescigno,G.,(1999)Effective Reduction of A Giant Left Atrium By Partial Autotransplantation, Annals of Thoracic Surgery, 67, 1164-1165.
View at Publisher | View at Google Scholar - Ece Tongug, Mert Kestelli, Ibrahim Ozsoyler, Levent Yilik, Arif Yilmaz, Cengiz Ozbek, Ayhan Akcay, Murat Yesil (2001)Limit of Indication For Plication of Giant Left Atrium, Asian Cardiovascular And Thoracic Annals, 9, 1
View at Publisher | View at Google Scholar - Yuda,A.,Nakatini,S.,Isobe,F., Kosakai,Y.,Miyataki,K., (1998)Comparative Efficacy of The Maze Procedure For Restoration of Atrial Contraction In Patients With And Without Giant Left Atrium Associated With Mitral Valve Disease, Journal of American College of Cardiology, 31, 1097-1102
View at Publisher | View at Google Scholar - Chen,M.,Chang,J, Chang, H.,(2004)Preoperative Atrial Size Predicts The Success of Radiofrequency Maze Procedure For Permanent Atrial Fibrillation In Patients Undergoing Concomitant Valvular Surgery, Chest, 125, 2129-2134
View at Publisher | View at Google Scholar - Kosaki,Y.,(2000) Treatment of Atrial Fibrillation Using Maze Procedure: The Japanese Experience, Seminars In Thoracic And Cardiovascular Surgery, 12, 44-52.
View at Publisher | View at Google Scholar - Schaff, H.,Dearani, J.,Daly,R., Orzulak,T.,Danielson, G.,(2000) Cox-Maze Procedure For Atrial Fibrillation: Mayo Clinic Experience, SemInars In Thoracic and Cardiovascular Surgery, 12, 30-37
View at Publisher | View at Google Scholar - Scherer,M.,Dzemali,O.,Aybec,T., Wimmer-Greinecker,G.,Moritz,A.,(2003)Impact of Left Atrial Size On Chronic Atrial Fibrillation In Mitral Valve Surgery, Journal of Heart Valve Disease, 12, 469-474.
View at Publisher | View at Google Scholar - Lim,C., Rhyu,W.,H.,Lee,Y.,Choh,J,H.,(2005) Management of Left Atrial Endocardium After Extensive Thrombectomy, Annals of Thoracic Surgery, 79, e11-e12.
View at Publisher | View at Google Scholar - Kim,S.,H.,Woo,S.,Y. Oh,Y.,K.,Chung,W.,B.,Lim,C.,H.,Shin,J,W.Park,C.,S.,Youn,H.,J,Chung, W.,S., Hong,S.,J,(2004) A Case of Recurrent Thrombus Associated With Left Atrial Calcification, Korean Circulation Journal, 34, 323-327,
View at Publisher | View at Google Scholar - Roberts,W.,C., Humphries,J,O.,Morrow,A.,G.,(1970) Giant Right Atrium In Rheumatic Mitral Stenosis: Atrial Enlargement Restricted By Mural Calcification, American Heart Journal, 79, 28-35.
View at Publisher | View at Google Scholar - Vallejo,J,L.,Merino,C., Gonzalez Santos,J,M, Bastida,E., Albertos,J,Riesgo,M.,J,Gonzalez De Diego,F.,(1995)Massive Calcification of The Left Atrium: Surgical Implications, Annals of Thoracic Surgery, 60, 1226-1229.
View at Publisher | View at Google Scholar - Yokoyama,K., Konno,K.,Suzuki,S., Isshiki,T.,(2007)”Serial Assessment of Liquefaction Necrosis of Mitral Annular Calcification, Echocardiography And Multislice Computed Tomography, Circulation, 115(1), e1-e2
View at Publisher | View at Google Scholar - Vilacosta,L., Gomez,J.,Almeria,C.,Castillo,J,A.,San Roman,J,A.,Zamorano, J,et al (1994)Massive Left Atrial Calcification: A Limitation of Transesophageal Echocardiography, American Heart Journal, 127, 461-463
View at Publisher | View at Google Scholar - Shinichi Tsumaru, Kenji Minakata, Kazuhiro Yamazaki, Masaki Nakamura, Hisashi Sakaguchi, Ryuzo Sakata (2015) Redo Mitral Valve Replacement In Patient With “Coconut Atrium”, Annals of Thoracic Surgery, 99,1454.
View at Publisher | View at Google Scholar - De Sanctis,R.,W., Dean,D.,C., Bland, E.,F.,(1964) Extreme Left Atrial Enlargement, Some Characteristic Features, Circulation, 29,14.
View at Publisher | View at Google Scholar - Johnson,J., Danielson,G.,L., Mac Vaugh, H., Joyner,C.,R.,(1967) Plication of Giant Left Atrium At Operation For Severe Mitral Regurgitation, Surgery, 61, 118.
View at Publisher | View at Google Scholar - Le Roux,B.,T.,Gotsman,M.,S., (1970) Giant Left Atrium, Thorax, 25, 190.
View at Publisher | View at Google Scholar - Tamura, Y., Nagasaka,S., Abe,T., Taniguchi,S.,(2008) Reasonable And Effective Volume Reduction Of A Giant Left Atrium Associated With Mitral Valve Disease Annals of Thoracic And Cardiovascular Surgery, 14, 252-255
View at Publisher | View at Google Scholar - Pablo M A Pomerantzeff (2013) Tangential Triangular Resection For Correction Of Giant Left Atrium, ISMICS (Annual Scientific Meeting- Invitation, Technologies, And Techniques In Cardiothoracic And Cardiovascular/Vascular Surgery), 12-15 June
View at Publisher | View at Google Scholar
