

case report | DOI: https://doi.org/10.31579/2835-7957/071
Gastric and Colonic Metastases of Breast Cancer
1Department of Gastroenterology, Jingmen People’s Hospital, Jingmen, China.
2The First College of Clinical Medical Science, China Three Gorges University, Yichang, China.
3Institute of Digestive Disease, China Three Gorges University, Yichang, China.
4Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, China.
*Corresponding Author: Wei Liu, Ph.D., Institute of Digestive Disease, China Three Gorges University, 8 Daxue Road, Yichang 443000, China.
Citation: Jian-Xin Zhang, Wei Liu., (2024), Gastric and Colonic Metastases of Breast Cancer, Clinical Reviews and Case Reports, 3(3); DOI:10.31579/2835-7957/182
Copyright: © 2024, Loubna Taali. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 March 2024 | Accepted: 20 March 2024 | Published: 28 March 2024
Keywords: thyroglossal tract cyst; adult; laryngocele
Abstract
The thyroglossal tract cyst (TTC) represents the most common congenital cervical mass, and it is mainly of interest to the pediatric population, with presentation in the form of a midline cervical mass. A recent lateralized or paramedian cervical mass occurring in an adult must first be eliminated as a malignant mass or laryngocele. We report the case of a 32-year-old young man, without any particular pathological history, who presented with a recent appearance of a right paramedian cervical mass adjacent to the thyroid cartilage. Preoperative CT scan revealed a cystic mass on the right, with a hemorrhagic component. Intraoperatively, the lesion was embedded in the infrahyoid muscles and it had connections with the anterior surface of the body of the hyoid bone. A Sistrunk procedure was performed. In most cases, a history and a meticulous physical examination are sufficient to make the diagnosis. The distinction between laryngocele and KTT must be made intraoperatively to avoid an inappropriate or incomplete surgical procedure. ENT surgeons must always expand the list of differential diagnoses when faced with a cervical cystic mass, in order to adapt the treatment in the event of an intraoperative surprise.
Introduction
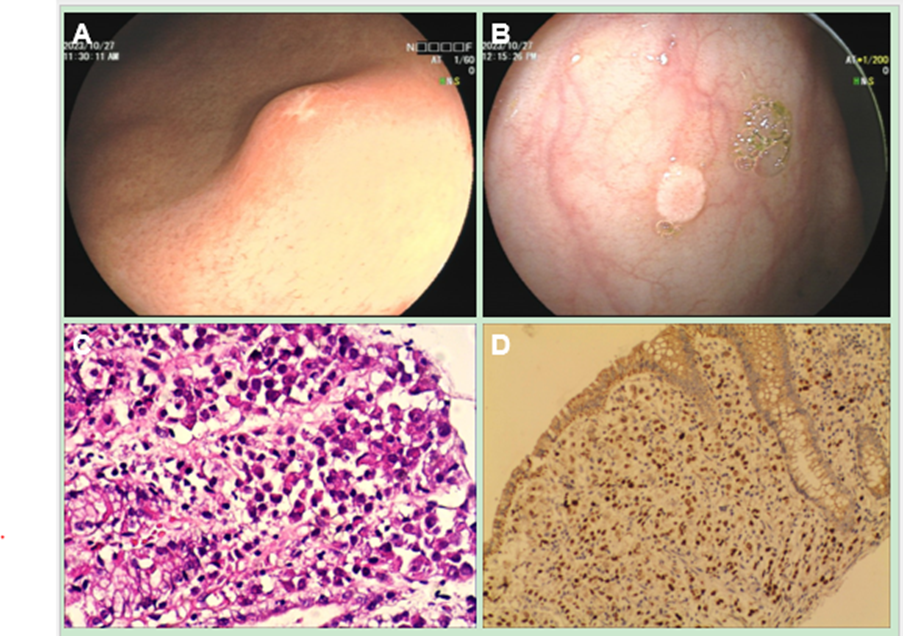
A 61-year-old woman presented with a 1-week history of weight loss and abdominal pain. Two years ago, she received a radical mastectomy and chemotherapy for breast cancer. She denied alcohol consumption and had no personal history of peptic ulcer. Laboratory tests and abdominal computed tomography (CT) were normal. Upper gastrointestinal endoscopy demonstrated a 1.2 cm in diameter, prominent nodule on the surface of the antrum of stomach (Figure 1A). A white, flat, elevated lesion 8 mm in size was identified at the ascending colon in screening colonoscopy (Figure 1B). A sessile serrated adenoma/polyp could not be excluded. Endoscopic mucosal resection was performed. Both gastric and colonic biopsies demonstrated infiltration by malignant cells of metastatic lobular breast carcinoma (Figure 1C). Immunohistochemical analysis indicated that tumor cells were positive for GATA3 (Figure 1D) and mammaglobin. These lesions were diagnosed as gastric and colonic metastases of breast cancer. The most common sites of metastases of breast cancer are bone, lung, liver, and brain. The metastatic spread of breast cancer to the stomach and colon commonly represents a diagnostic challenge. Both gastric and colonic metastases are rare. Nonspecific symptoms and various appearances of metastatic lesions may confuse the diagnosis. A high index of suspicion for potential breast cancer metastasis to the digestive tract should be maintained when new gastrointestinal symptoms develop in patients with a history of breast cancer. [1-3]
Acknowledgements
Footnote
Conflicts of Interest:
The authors have no conflicts of interest to declare.
Ethical Statement:
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “GI Image”. Board institutional approval was not required.
Author’s contributions
Collection of data and writing: Wei Liu.
Manuscript preparation: Jian-Xin Zhang.
Final approval of the manuscript: Wei Liu.
References
- Ben Kridis W, Lajnef M, Fki A, Belaid L, Khanfir A. An uncommon case of synchronous gastric and colonic metastases from breast cancer. JGH open : an open access journal of gastroenterology and hepatology. 2022;6(8):587-9. doi:10.1002/jgh3.12784.
View at Publisher | View at Google Scholar - Arif FZ, Breese RO, Burke R. Breast Cancer Metastasis to Colon. The American surgeon. 2023:31348231173979. doi:10.1177/00031348231173979.
View at Publisher | View at Google Scholar - Takedomi H, Akutagawa T, Sakata Y. Colon Metastasis of Breast Cancer With a Unique Endoscopic Finding. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2020;18(7):e74. doi:10.1016/j.cgh.2019.04.014.
View at Publisher | View at Google Scholar
