

Research Article | DOI: https://doi.org/10.31579/2834-5126/145
First Long-Term, Eleven-Year, Parasitological Surveys, During a Village-Scale Malaria Vector Control Program in Angola
1Director of Research, Jalan Raya Sakah, Batuan, Sukawati, Bali, Indonesia, 80582.
2 OCEAC (Organisation of Coordination for Endemic Diseases Control in Central Africa), Yaoundé Cameroon.
3Malaria Control Program, Medical Department, Sonamet, Lobito, Angola.
4Hygiene Safety Environment, Batuan, Bali Indonesia.
*Corresponding Author: Carnevale Pierre., Director of Research, Jalan Raya Sakah, Batuan, Sukawati, Bali, Indonesia, 80582.
Citation: Pierre C., Toto Jean-Claude., Franck M., Guillaumed M., (2026), First Long-Term, Eleven-Year, Parasitological Surveys, During a Village-Scale Malaria Vector Control Program in Angola, Clinical Trials and Clinical Research,5(4); DOI:10.31579/2834-5126/145
Copyright: © 2026, Carnevale Pierre. This is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 April 2026 | Accepted: 16 April 2026 | Published: 11 May 2026
Keywords: angola; vector control at village-scale level with four methods; long-lasting insecticide-treated nets; insecticide-treated plastic sheeting; inside residual spraying
Abstract
Abstract
Objectives
At the request, and with the National Malaria Control Program of Angola (NMCPA), a comprehensive program was planned, and implemented, in villages around Balombo town (Benguela Province) with two objectives: to compare, in natural conditions, the efficacy of four methods of vector control; and to check for any parasitological rebound effect several years after vector control.
Patients and Methods
Four vector control methods were implemented: long-lasting deltamethrin treated nets (LLIN), PermaNet®2.0 (P2) alone; P2 combined with deltamethrin insecticide-treated plastic sheeting (ITPS) model ZeroFly®; ITPS model ZeroVector® alone, and two rounds of lambdacyhalothrin indoor residual spraying (IRS) followed by ITPS installation. Each method was implemented in one village. Several analyses of short-term entomological, parasitological, and immunological impact had already been published. The long-term, eleven years, parasitological evaluation was performed in these four villages, and was based upon regular cross-sectional surveys on random samples of volunteer’s asymptomatic children ≤15-year-old. Thick blood films were made in the field, and examined by optical microscope in the medical department of the Angolese Sonamet® Company in Lobito which implemented, and supported, its Malaria Control Program (MCP) in Benguela Province. The Balombo program was a part of this MCP. Three parasitological indicators were analyzed: Plasmodium parasite prevalence, parasite load and gametocyte index.
Results
From the year 2007 to the year 2018, 136 parasitological cross-sectional surveys were performed. 12,525 thick blood films (TBF) were prepared. Plasmodium were observed in 2,392 TBF, i.e., a parasite prevalence of 19.1%, and gametocytes in 247 blood films, i.e., a gametocyte rate of 1.97%. Parasite prevalence (PP) for the two years before vector control (years 2007-2008) (PP=39.4%; n=4,302) and the nine years after (years 2009-2018) (PP=8.5%; n=8,223) showed a significant 78.4% decrease. This decrease was similar with all four methods: -77.8% with treated nets alone; -76.9% with the combination nets + ITPS ZeroFly®; -80.8% with ITPS ZeroVector® alone; and -76.8% with indoor spraying followed by ITPS installation. After vector control there was observed an evolution of the parasite prevalence in three successive steps: first an important drop of 61% the first year following vector control and another 64% the following year. Then, over several years, occurred a plateau, which remained at a low parasite prevalence level (< 5%) until the 2015 national malaria outbreak, which induced an increase of the parasite prevalence. But, even during this time, the parasite prevalence (PP=17.8%; n=991) was still significantly lower than before vector control. The impact of the national malaria outbreak was also clearly observed on the parasite load which increased significantly. The gametocyte index, and the parasite load, had the same “three steps” evolution as parasite prevalence after vector control. The several years of low plasmodial infections were a crucial epidemiological indication. No rebound effect of parasite prevalence was noticed ten years after vector control.
Conclusion
The four methods of vector control similarly reduced Plasmodium prevalence, gametocyte index, and parasite load. Ten years after vector control, the parasite prevalence was still lower than before vector control despite the national malaria outbreak and no rebound was noticed. During the malaria outbreak it was observed a significant increase of the parasite load which could be matter of concern. Actual community participation, observed during ITPS installation inside their homes, was a crucial point for the sustainability, and therefore efficacy, of this vector control method. Therefore, ITPS alone, or in combination with treated-nets, could be recommended, as an additional complementary, tool in the arsenal of the National Malaria Control Program of Angola, and other countries.
Introduction
According to a WHO World Malaria Report, malaria is still a major public health concern in Angola (37 million of inhabitants) with 8 251 449 estimated malaria cases and 16,169 estimated deaths in 2023 [1] « The accuracy of malaria prevalence estimates in Angola has traditionally been somewhat compromised by incomplete reporting, inability to test due to stockouts of the necessary materials, and other logistic challenges, such as transportation of materials to remote areas and efficient distribution. » [2-5]. The situation is worsening with drugs resistant P. falciparum [6-8] and the National Malaria Control Program of Angola (NMCPA) developed a comprehensive program, including intermittent preventive treatment for pregnant women 9 and the use of ACTs as first line treatment of uncomplicated malaria. [10-12]. A special accent was given to vector control, but due to the failure of inside residual spraying [13], the program has focused on large-scale distributions of insecticide-treated nets. (ITN/LLIN) [14, 15] Recent studies showed that one year after distributions the ITN coverage dropped from 98% to 63% [16] “indicating that new ITNs/LLINs must be continuously supplied to replace those that have lost efficacy and are torn, in order to maintain high levels of coverage. » 2 But, in Angola, as elsewhere, there is a problem of non-use, or misuse, or re-use of nets. [17-19]. Surveys in village around Balombo reported that it two or-three years, most of distributed LLINs were withdrawn, 20 and, simultaneously, parasite prevalence increased. One of the key points for the success of a malaria vector control is its sustainability, which depends, among other things, on actual community participation [21], the tools selected, the insecticide resistance, and the availability resources in the short, middle and long term. A “malaria disaster” was feared with the spread of pyrethroid resistance [22-24], which could contribute to reduced efficacy of insecticide-treated nets 25, as could other factors. [26] It was proposed to combine pyrethroid treated long-lasting nets with indoor residual spraying [27,28] with other classes of insecticide, or to combine two different insecticides on the same nets, [29] or to add on (or in) the nets a synergist such as piperonyl butoxide [30-35], or juvenile hormone analog such as pyriproxyfen, 36-40 or chlorfenopyr 41-46 and this could increase the price of the net. According to these difficulties in LLINs, in term of implementation, efficacy and sustainability, it clearly appeared a need for new tools, and the recently developed insecticide-treated plastic sheeting (ITPS) seemed to be an interesting option for malaria control. 47-49 Treated with pyrethroid they were of great efficacy in refugee camps 47, or combined with LLIN 50 or treated with carbamates and then combined with LLIN 51, 52 or treated with organophosphate. [53] Therefore, combining treated nets and ITPS (or IRS) seemed to be an interesting approach. [54, 55] Considering their reported efficacy, and acceptability, 56 ITPS appeared worthy of epidemiological evaluation in villages around Balombo town as the acceptability of ITPS had already been observed in the close town of Huambo. [57]. The project was a part of the current Malaria Control Program of the Sonamet® Angolese Company, it was requested by the National Malaria Control Program of Angola, which gave clearance and support; the public health department of the Benguela province was actually involved in field surveys. The project had two objectives: to comprehensively compare the feasibility, and efficacy, of four methods of vector control, each one in one village, in completely natural conditions, without disturbing other measures implemented in the region by National or Non-Governmental Organizations [58-59]. The second objective was to check for any long-term negative parasitological impact, called “rebound effect”, meaning a sharp increase of plasmodial infections which could occurred several years after vector control, supposed to have decrease immunity.
II. Methods
The ecological and social situations of Balombo area (Benguela Province, Angola) (12° S; 14° E) and the villages studied were already presented [58, 59]. The villages for the Balombo trial were selected by the National Malaria Control Program of Angola, they far each other to avoid any “contamination” of mosquitoes going from one to another one village and influencing catches samples.
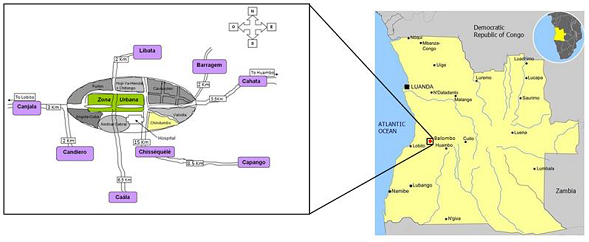
Map of the area. From Brosseau et al [58]
The demographic situation, tools for vector control and the flow diagram of vector control implementation are presented in Table 1.
Village | Number of inhabitants | Number of houses | Number of sleeping units* |
Cahata | 517 | 154 | 442 |
Capango | 177 | 60 | 89 |
Barragem | 620 | 134 | 168 |
Candiero | 654 | 191 | 380 |
Total | 1,968 | 539 | 1,079 |
Table 1: Demographic information on the four villages involved, at the beginning of the project in February 2007. (* a sleeping unit was defined as any item used for sleeping, including permanent beds, temporary mats, cardboard, loincloths, and other items unfolded at night to sleep.)
Each one of the four villages of this study received one vector control method only, with complete coverage of each house which were already numbered and geo-localized following classical protocol for planning, implementing and monitoring vector control operations 60. This approach was used to identify house with “at least” one member having a positive thick blood films at each survey and localize eventual “hot spot 61
Four tools were used for vector control:
- Long-lasting insecticide-treated nets (LLIN), model “PermaNet® 2.0”, treated at 55 mg a.i. deltamethrin (δ)/m2; with a surface area of 13 m2, the total amount of insecticide was 0.715 gr a.i. deltamethrin/LLIN.
- Insecticide-treated plastic sheeting (ITPS), model “ZeroVector” ® (ZV) treated at 170 mg a.i. δ/m2 and presented in rolls.
- Insecticide-treated plastic sheeting, model “ZeroFly®” (ZF), treated at 360 mg a.i. δ/m2; with a size of 19.11 m2, the total amount of insecticide was 6.88 gr a.i. δ/ ZeroFly®.
- Sachets of lambdacyhalothrin (λ) “Icon® WP”, 6.25 gr a.i. λ/sachet for indoor residual spraying, (IRS) targeting 25 mg a.i./m2 of sprayed surface, two rounds, followed by installation of ITPS.
Full coverage in LLIN, ITPS, and the first round of IRS were achieved in December 2008. (Table 2)
Village | February 2007 | February 2008 | December 2008 | June2009 | January 2010 |
Cahata
| P 2.0 LLIN 310 LLIN given | P2.0 LLIN 195 LLIN given | P2.0 LLIN 25 LLIN given | xx | xx |
Capango | C | C | 93 P2.0 LLIN given + 93 P2.0 ITPS ZF (1,209 m2) | xx | xx |
Barragem | C | C | 5,554 m2 ITPS ZV | xx | xx |
Candiero | C | C | λIRS round1 191 houses treated Surface treated: 9,500 m2 | λIRS round2 176 houses treated Surface treated: 8,750 m2 | δITPS
Surface treated: 4,914 m2 |
Table 2: Vector control operations in the four villages of the trial. C= control village, without any vector control operation implemented; xx = no intervention; LLIN = long-lasting insecticide treated net PermaNet 2.0; ITPS= insecticide-treated plastic sheeting; ZF = ITPS model ZeroFly®; ZV= ITPS model ZeroVector®; IRS= inside residual spraying; m2= covered surface; δ=deltamethrin; ʎ=lambdacyhalothrin).
In Cahata it was given 530 LLINs P.2.0 for 154 houses and 442 sleeping units assuming a complete coverage. In Capango it was given 93 LLINs P2.0 for 60 houses and 89 sleeping units assuming also a complete coverage. The parasitological follow-up was scheduled to occur for 11 years; the first parasitological survey was done in February 2007 and the last in February 2018. Long-term parasitological study was based on regularly done cross-sectional surveys (CSS) for each survey58, to get parasite prevalence on randomly selected volunteer’s asymptomatic children≤15-year-old in the four villages. Thick blood films (TBF) were done, and colored in the field, then examined with optical microscope in the medical department of the Angolese Sonamet® Company in Lobito, with double-check of 10% of TBF in the parasitological laboratory of OCEAC in Yaoundé. Plasmodium species were determined, and counted, compared to 200 white blood cells (WBC) then estimated for 1 ml of blood (assuming 8,000 WBC/ml of blood). Three classical indicators were analyzed: Plasmodium prevalence, parasite load and gametocyte index. For statistical analyses all Plasmodium infections were combined as P. malariae, P. ovale, and P. vivax, were scarcely diagnosed, and often associated with P. falciparum. Results were given to the village health worker, in each village, for action according to the National Malaria Control Program of Angola (NMCPA). Percentages were compared using the classical Chi square, while parasitaemia distributions were analyzed using the Mann-Whitney nonparametric test, and GraphPad software.
III. Results
From year 2007 to year 2018, 136 parasitological cross-sectional surveys (CSS) were done; 12,525 thick blood films (TBF) were prepared. Plasmodium were microscopically observed in 2,392 blood films, i.e., a parasite prevalence of 19.1%, and gametocytes in 247 blood films, i.e., a gametocyte rate of 1.97%, i.e. around 10 times less than parasite prevalence.
III-1. Plasmodial infections in Cahata village (with LLIN)
III-1-1. Plasmodium prevalence
35 surveys (CSS) were done; 3,665 thick blood films were prepared. Plasmodium were observed in 880 blood films (parasite prevalence=24.0%) and gametocytes in 100 blood films (gametocyte index=2.73%). (Table 3)
Cahata | TBF+ | n | PP | G+ | GI |
Y 2007 | 408 | 739 | 55.2% | 35 | 4.7% |
Y 2008 | 242 | 675 | 35.9% | 36 | 5.3% |
Y 2009 | 108 | 534 | 20.2% | 11 | 2.1% |
Y 2010 | 45 | 580 | 7.8% | 6 | 1.0% |
Y 2011 | 6 | 125 | 4.8% | 6 | 4.8% |
Y 2012 | 5 | 413 | 1.2% | 1 | 0.2% |
Y 2013 | 4 | 256 | 1.6% | 0 | 0.0% |
Y 2014 | 3 | 70 | 4.3% | 0 | 0.0% |
Y 2015 | 22 | 158 | 13.9% | 0 | 0.0% |
Y 2016 | 11 | 36 | 30.6% | 3 | 8.3% |
Y 2018 | 26 | 79 | 32.9% | 2 | 2.5% |
Total | 880 | 3,665 | 24.0% | 100 | 2.7% |
Table 3: Yearly evolution of parasite prevalence in asymptomatic children ⋜ 15-year-old in Cahata village (TBF= thick blood films, n= number of TBF examined; PP= parasite prevalence; G+= thick blood films with gametocytes; GI= gametocyte index).
For parasite prevalence a significant decrease of 35% occurred after the first distribution of nets (from 55.2%; n=739 to 35.9%; n=675), then -44?ter the full coverage in nets (PP=20.2%; n=534 in year 2009) (Annex 1). The decrease still occurred the following years (Table 3) with a plateau at a low level (⋜5%) until the outbreak of 2015. (Figure 1).
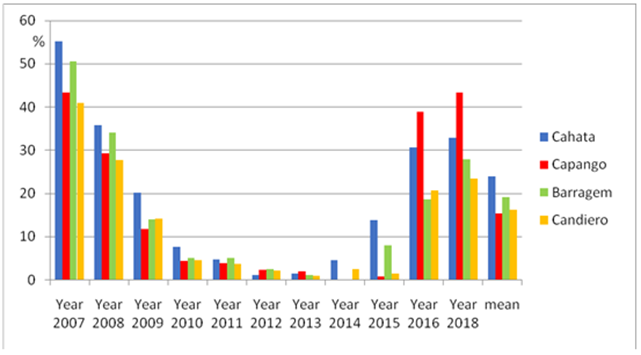
Figure 1: Yearl evolution of parasite prevalence in asymptomatic children ⋜15-year-old in each village.
Between the two first years, 2007-2008 (called “before” vector control) with a parasite prevalence of 46% (n=1,414) and the following nine years (2009-2018), called “after” vector control, the decrease of 78% was striking (PP=10.2%; n=2,251). For the three years of the malaria outbreak (2015-2018) the parasite prevalence (PP=21.6%; n=273) was significantly two times lower than at the beginning of the trial.
III-1-2. Plasmodium load
The parasite load (Figure 2):
- significantly decreased after the first distribution of treated nets (P-value<0.0001 between 2007 and 2008), increased after the second distribution of nets (P value= 0.0036 between 2008 and 2009);
- significantly decreased after distribution of nets for full coverage (P-value= 0.0216 between 2009 and 2010);
- remained very low during four years, until 2015 when it significantly increased at the time of the national malaria outbreak (P value= 0.0035) and remained relatively high despite measures implemented by the National Malaria Control Program and other organizations.
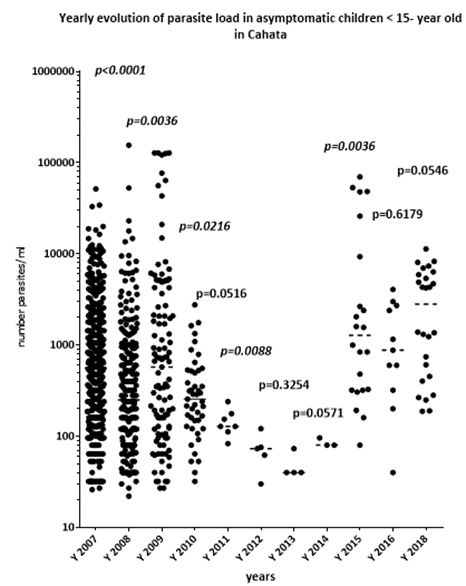
Figure 2: Yearly evolution of parasite load in asymptomatic ⋜15-year-old children in Cahata. (the statistically significant P values are in italics; --- = median value)
The four years of low parasite load is noteworthy.
III-1-3. Gametocyte index
The gametocyte index (GI), significantly decreased after full distribution of nets, and remained at a low level over four years (Figure 3).
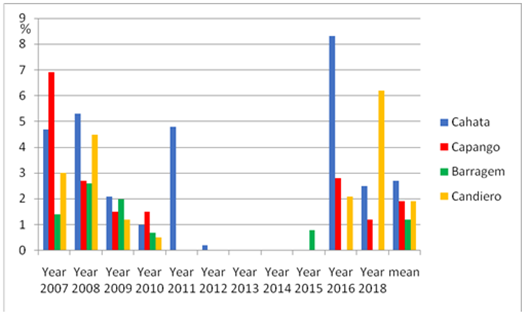
Figure 3: Yearly evolution of gametocyte index in asymptomatic children⋜15-year-old in each village.
In February 2018, i.e., 11 years after the first distribution of nets, the gametocyte index was about two times less than in February 2007, before any intervention (respectively 2.5%; n=79 and 4.7%; n=738), the same
twofold decrease as for parasite prevalence. Even during the malaria outbreak period, the gametocyte index (1.83%; n=273) was significantly lower than before vector control, (5.02%; n=1,414) (χ2= 5.41; p-value= 0.020; OR= 0.35 [0.12-0.92]).
III-2. Plasmodial infections in Capango village (with nets and ITPS « Zero Fly® »)
III-2-1. Plasmodium prevalence
33 surveys were done; 2,388 thick blood films were prepared; Plasmodium were observed in 370 blood films (parasite prevalence=15.5%) and gametocytes in 45 blood films (gametocyte index =1.88%). (Table 4)
Capango | TBF+ | n | PP | G+ | GI |
Y 2007 | 119 | 274 | 43.3% | 19 | 6.9% |
Y 2008 | 110 | 376 | 29.3% | 10 | 2.7% |
Y 2009 | 55 | 466 | 11.8% | 7 | 1.5% |
Y 2010 | 21 | 466 | 4.5% | 7 | 1.5% |
Y 2011 | 5 | 128 | 3.9% | 0 | 0.0% |
Y 2012 | 6 | 251 | 2.4% | 0 | 0.0% |
Y 2013 | 3 | 143 | 2.1% | 0 | 0.0% |
Y 2014 | 0 | 57 | 0.0% | 0 | 0.0% |
Y 2015 | 1 | 108 | 0.9% | 0 | 0.0% |
Y 2016 | 14 | 36 | 38.9% | 1 | 2.8% |
Y 2018 | 36 | 83 | 43.4% | 1 | 1.2% |
Total | 370 | 2,388 | 15.5% | 45 | 1.9% |
Table 4: Yearly evolution of parasite prevalence in asymptomatic children ⋜ 15-year-old in Capango village (TBF= thick blood films, n= number of TBF examined; PP= parasite prevalence; G+= thick blood films with gametocytes; GI= gametocyte index).
The yearly evolution of parasite prevalence (Figure 1) showed:
- a significant natural decrease (by 33%) from year 2007 to 2008; for these two years without intervention the overall parasite prevalence was 35.2% (n=650);
- then a striking drop of 60% in 2009, the first year after implementation of vector control;
- a decrease maintained the following years: -62% in 2010, then -13% in 2011;
- a plateau at a low level (<5%) until 2015, i.e., seven years after vector control implementation;
- a sharp increase in 2016, and the years after, showing an obvious impact of the national malaria outbreak.
But even during this period, the parasite prevalence (PP=22.5%; n=227) was significantly lower than before vector control (PP=35.2%; n=650) (χ2= 12.6; OR= 0.53 [0.37-0.76]) (Annex 2).
Ten years after vector control, no “rebound effect” of the parasite prevalence was observed.
III-2-2. Plasmodium load
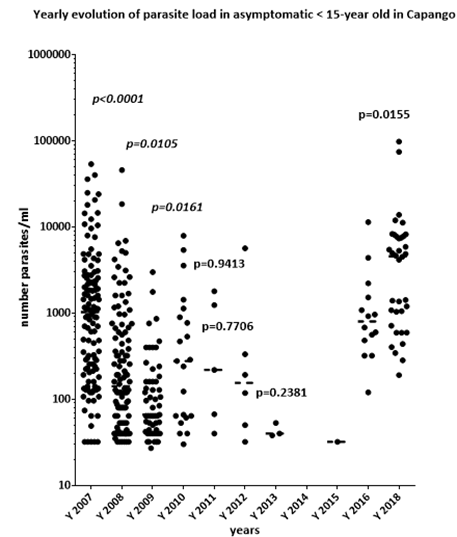
Figure 4: The distributions of parasite load from year 2007 to year 2018 are plotted in statistically significant P values are in italics; --- = median value).
A significant reduction occurred in 2009, the first year after implementation of the combination of LLINs and ITPS ZeroFly®; then a curious increase in 2010, followed by a striking reduction over four years with a low level of parasite load until 2015.
The impact of the national malaria outbreak was striking in 2016 and 2018, with a significant increase in 2018 (higher than in 2007: P-value =0.0005; and in 2008: P-value <0.0001), but the parasite load in 2016 was similar to 2007 (P-value= 0.9465).
III-2-3. Gametocyte index
The impact on gametocyte index of the combination of LLIN and ZeroFly® installed inside every house was striking (Figure 3), with five years without detecting any gametocytes in thick blood films. In 2018, the gametocyte index decreased while both parasite prevalence and parasite load increased.
It is worth considering the evolution of the gametocyte index (GI) during three successive periods:
- before vector control: GI=4.46% (n=650);
- after vector control but before malaria outbreak (GI= 0.93% (n=1,511);
- during malaria outbreak: GI= 0.88% (n=227), i.e., 80% less than before vector control.
This clearly shows the long-term impact of this vector control method on gametocyte index in this village.
III-3. Plasmodial infections in Barragem village (insecticide-treated plasting sheeting, Zero Vector® only)
III-3-1. Plasmodium prevalence
35 surveys were done, 3,042 thick blood films (TBF) were prepared, Plasmodium were observed in 584 TBF, i.e., a parasite prevalence of 19.2%, while gametocyte were observed in 38 TBF, i.e., a gametocyte index of 1.25% (Table 5).
Barragem | TBF+ | n | PP | G+ | GI |
Y 2007 | 215 | 428 | 50.5% | 6 | 1.4% |
Y 2008 | 213 | 622 | 34.2% | 16 | 2.6% |
Y 2009 | 75 | 536 | 14.0% | 11 | 2.0% |
Y 2010 | 30 | 585 | 5.1% | 4 | 0.7% |
Y 2011 | 7 | 136 | 5.1% | 0 | 0% |
Y 2012 | 7 | 265 | 2.6% | 0 | 0% |
Y 2013 | 2 | 172 | 1.2% | 0 | 0% |
Y 2014 | 0 | 69 | 0% | 0 | 0% |
Y 2015 | 10 | 125 | 8.0% | 1 | 0.8% |
Y 2016 | 8 | 43 | 18.6% | 0 | 0% |
Y 2018 | 17 | 61 | 27.9% | 0 | 0% |
Total | 584 | 3,042 | 19.2% | 38 | 1.2% |
Table 5: Yearly evolution of parasite prevalence in asymptomatic children ⋜ 15-year-old in Barragem village (TBF= thick blood films, n= number of TBF examined; PP= parasite prevalence; G+= thick blood films with gametocytes; GI= gametocyte index).
The evolution of parasite prevalence (Figure 1) had the same general trend as in other villages, with:
- a natural and significant drop of 32% the first two years; for this period (“control”) the overall parasite prevalence was 40.8% (n=1,050);
- a significant drop of 59?tween 2008 and 2009, i.e. the first year after implementation of vector control, and another significant drop of 63% the second year (2010) (Annex 3);
- a noteworthy five years with a very low level of parasite prevalence of <5%;
- an increase in 2015, then 2016, and 2018 linked to the national malaria outbreak; during these three years the parasite prevalence was 15.3% (n=229), i.e., 62% lower (significantly) than before vector control. For the period after vector control the parasite prevalence was 7.8% (n=1,992), also significantly lower than before intervention (-81%).
In Barragem also, 10 years after vector control based on the installation of only ITPS on the walls of villagers' houses no “rebound” of the parasite prevalence was observed despite the malaria outbreak.
III-3-2. Plasmodium load
The parasite load (Figure 5):
- significantly naturally decreased the first two years, from 2007 to 2008 (P-value< 0.0001);
- was similar in 2008 (before vector control) and 2009 (after vector control) (P-value= 0.2778);
- was similar between 2009 and 2010 (P-value= 0.1775); and in 2010 and 2011 (P-value= 0.52);
- was significantly lower in 2012 than in 2011 (P-value =0.041);
- significantly increased in 2015 compared to 2007 (P-value= 0.0282);
- then remained at a similar level between 2015 and 2016, (P-value= 0.7418); and between 2016 and 2018, (P-value= 0.3088);
- in 2012, i.e., four years after the installation of wall lining in the houses of Barragem, the parasite load was significantly lower than in 2008, before installation (P-value= 0.0036);
- parasite load remained very low even in 2013 and 2014, i.e., six years after vector control and it significantly increased with the malaria outbreak.
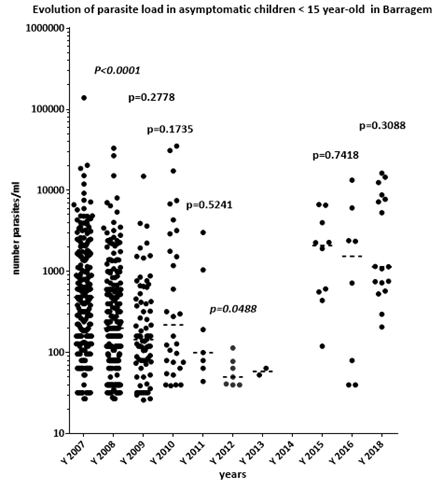
Figure 5: Yearly evolution of parasite load in asymptomatic ⋜15-year-old children in Barragem. (the statistically significant P values are in italics).
III-3-3. Gametocyte index
For the two years before vector control the overall gametocyte index (GI) was 2.1% (n=1,050). It remained at this level of approximately 2% the first year after implementation of vector control, then, and for the eight following years; it remained at a very low level, (Figure 3) with only one gametocyte carrier detected among the 871 thick blood films made between 2011 and 2018.
III-4. Plasmodial infections in Candiero village (two rounds of IRS then ITPS)
III-4-1. Plasmodium prevalence
33 surveys were done, 3,430 thick blood films were prepared, Plasmodium were observed in 558, i.e., parasite prevalence= 16.3%, and gametocytes in 64 blood films, i.e., gametocyte index= 1.86% (Table 6).
Candiero | TBF + | n | PI | G+ | GI |
Y 2007 | 180 | 439 | 41,0% | 13 | 3,0% |
Y 2008 | 208 | 749 | 27,8% | 34 | 4,5% |
Y 2009 | 94 | 656 | 14,3% | 8 | 1,2% |
Y 2010 | 29 | 629 | 4,6% | 3 | 0,5% |
Y 2011 | 5 | 131 | 3,8% | 0 | 0,0% |
Y 2012 | 7 | 305 | 2,3% | 0 | 0,0% |
Y 2013 | 2 | 181 | 1,1% | 0 | 0,0% |
Y 2014 | 2 | 78 | 2,6% | 0 | 0,0% |
Y 2015 | 2 | 133 | 1,5% | 0 | 0,0% |
Y 2016 | 10 | 48 | 20,8% | 1 | 2,1% |
Y 2018 | 19 | 81 | 23,5% | 5 | 6,2% |
Total | 558 | 3,430 | 16,3% | 64 | 1,9% |
Table 6: Yearly evolution of parasite prevalence in asymptomatic children ⋜ 15-year-old in Candiero village (TBF= thick blood films, n= number of TBF examined; PP= parasite prevalence; G+= thick blood films with gametocytes; GI= gametocyte index).
The yearly evolution of parasite prevalence (Figure 1) showed:
- a natural, but significant decrease of 32% during the two years before vector control (Annex 6), and for these two years “control” the parasite prevalence was 32.7% (n=1,188);
- a sharp significant decrease of 48% in 2009, the year with implementation of the two rounds of indoor residual spraying (in January then in June);
- a significant 68?crease in 2010, with installation of insecticide-treated plastic sheeting in January;
- a stabilization of parasite prevalence the following two years (PP= 23.5% in year 2018);
- during the three years of malaria outbreak the parasite prevalence was 11.8% (Annex 4)
- In Candiero also, even with the national outbreak of malaria, Plasmodium prevalence did not present any “rebound” many years after vector control implementation.
III 4-2. Plasmodium load
The parasite load was similar during the two “control” years (while the parasite prevalence significantly decreased). The following years, the reducing parasite load with complete vector control implementation was statistically significant (Figure 6).
The impact of the national malaria outbreak on the parasite load was clear in 2015, 2016, and 2018, with a significant increase, compared to period before vector control:
- between 2007 and 2016: P-value= 0.025;
- between 2007 and 2018: P-value< 0.0001;
- between 2008 and 2016: P-value= 0.0185;
- between 2008 and 2018: P-value< 0.0001.
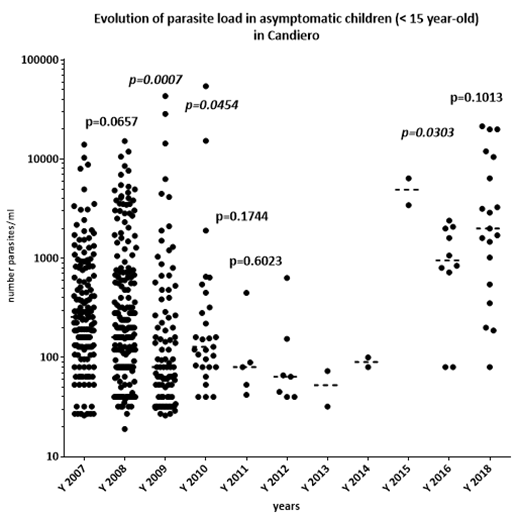
Figure 6: Yearly evolution of parasite load in asymptomatic ⋜15-year-old children in Candiero. (the statistically significant P values are in italics).
It is important to note how information could be different when considering either parasite prevalence or parasite load. The first two years, prevalence decreased but parasite load was the same. During the outbreak period, parasite prevalence was lower than before vector control, while parasite load statistically increased:
- year 2007 versus year 2018: p-value =0.0010 (significant difference)
- year 2008 versus year 2018: p-value < 0.0001 (significant difference)
III-4-3. Gametocyte index
The gametocyte index dropped significantly (by 80.7%) before, and after vector control, from 3.95% (n=1,188) to 0.76% (n= 2,242) (χ2= 43.4; OR=0.18 [0.11-0.32]) and it remained undetectable (with the size of the sample) for five years (Figure 3) before the important increase in 2018 due to the national malaria outbreak. The key point is this very low level of human infectivity for vectors for several years.
III-5. Synthesis
In term of parasite prevalence, the four methods of vector control induced (Table 7):
- a similar trend in the long-term evolution of parasite prevalence (Figure 1);
- a significant drop by 78.5% for the nine following years after vector control, (PP= 8.5%; n= 8,223);
- a similar overall decrease: -77.8% with LLINs; -76.9% with the combination of LLIN and ITPS; -80.8% with ITPS alone; -76.8% with the sequence IRS then ITPS
- a sharp, and significant, decrease the first and second year after implementation of vector control;
- a six-year “plateau” at a very low level (⋜5%);
- an increase, from year 2015, due to the national malaria outbreak (Figure 7). But even during this period the parasite prevalence (PP= 17.8%; n=991) was lower than before vector control (PP= 39.4%; n=4,302)
Village |
| Before |
|
| Between |
|
| Outbreak |
|
| TBF+ | n | PP | TBF+ | n | PI | TBF+ | n | PP |
Cahata | 650 | 1,414 | 46.0% | 171 | 1,978 | 8.6% | 59 | 273 | 21.6% |
Capango | 229 | 650 | 35.2% | 90 | 1,511 | 6.0% | 51 | 227 | 22.5% |
Barragem | 428 | 1,050 | 40.8% | 121 | 1,763 | 6.9% | 35 | 229 | 15.3% |
Candiero | 388 | 1,188 | 32.7% | 139 | 1,980 | 7.0% | 31 | 262 | 11.8% |
Total | 1,695 | 4,302 | 39.4% | 521 | 7,232 | 7.2% | 176 | 991 | 17.8% |
Table 7: Evolution of parasite prevalence, by village, and period of the trial: Before= years 2007-2008; Between = years 2009-2014; Outbreak= years 2015-2018.
The longer lasting impact seemed having been obtained by the combination of LLIN and ZF, and the combination of IRS then ITPS.
Another key result, which must be highlighted, is the fact that, in the natural condition of the project, regardless of events and methods of vector control, no significant rebound effect on the parasite prevalence was noted several years after vector control implementation except the increase due to the national malaria outbreak.
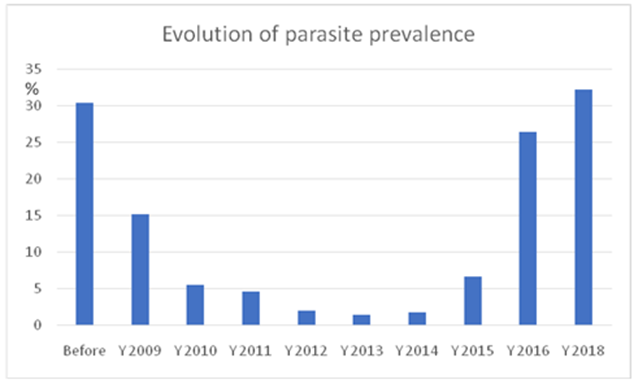
Figure 7: Overall evolution of parasite prevalence in asymptomatic children ⋜15-year-old before, and after, vector control in the four villages studied.
In term of gametocyte index: unlike plasmodic index the evolution of gametocyte was different depending on the vector control method implemented. (Table 8)
Period |
| Before |
|
| After |
| Diff |
| Outbreak |
|
Village | G+ | n | GI | G+ | n | GI |
| G+ | n | GI |
Cahata | 71 | 1,414 | 5.12% | 29 | 2,251 | 1.29% | -74.3% | 5 | 273 | 1.83% |
Capango | 29 | 650 | 4.46% | 16 | 1,738 | 0.92% | -79.4% | 2 | 227 | 0.88% |
Barragem | 22 | 1,050 | 2.09% | 16 | 1,992 | 0.80% | -61.7% | 1 | 229 | 0.44% |
Candiero | 47 | 1,188 | 3.95% | 17 | 2,242 | 0.76% | -80.7% | 6 | 262 | 2.29% |
Total | 169 | 4,302 | 3.93% | 78 | 8,223 | 0.95 | -75.4% | 14 | 991 | 1.42% |
Table 8: Evolution of gametocyte index, by village, and period of the trial. Before= years 2007-2008; Between = years 2009-2014; Outbreak= years 2015-2018.
It was observed peak in Cahata not observed in other villages (Figure 3), but a low level spanning several years was clear. (Figure 8).
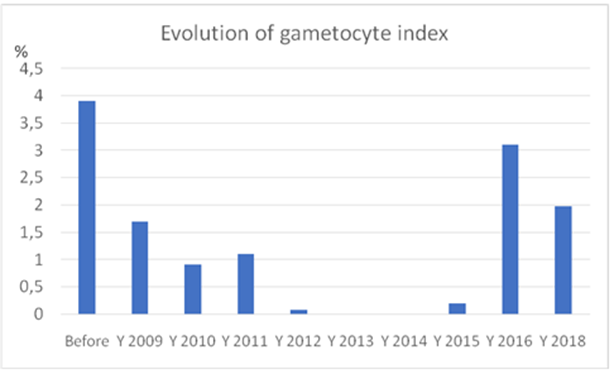
Figure 8: Overall evolution of the overall gametocyte index in asymptomatic children ⋜15-year-old before (years 2007-2008) and after vector control in the four villages studied.
Comparing the situation “before” and “after” vector control, the gametocyte index decreased by 74.3% in Cahata; 79.4% in Capango; 61.7% in Barragem; and 80.7% in Candiero, for a significant average reduction of 75.4% (χ2=129; OR=0.23 [0.18-0.31]). The level of reduction of plasmodial infection (before versus after vector control), on a long-term basis, was similar for parasite prevalence (-78%), and gametocyte index (-76%). In term of parasite load the several years with low parasite load, obtained similarly by each vector control method, is an important epidemiological output of the trial. But the influence of the malaria outbreak on the parasite load, which increased significantly, was clearly observed in the four villages. This confirmed the need for the sustainability of vector control implementation.
IV. Discussion
As was well underlined recently, “progress in the fight against malaria has stalled in recent years, highlighting the importance of new interventions and tailored approaches. A critical factor that must be considered across contexts and interventions is human behavior” 21 with “factors such as acceptance of insecticide-treated nets (ITNs) and indoor residual spraying (IRS), ability and willingness to consistently use and appropriately care for ITNs and refraining from post-spray wall modifications can all impact the success of core vector control interventions.” Sustainability, one of the keys to the success of malaria vector control, starts with the acceptability of the measures by population. This point was well studied in the area of Huambo, a town close to Balombo, and elsewhere, to gauge the acceptability of ITPS. [49, 56- 57] It was recently reported that “Integrated Vector Management (IVM) suggests making use of the full range of vector control tools available” and “the research needed to improve the quality and delivery of mosquito vector control should focus on (among other) the development of effective and eco-friendly tools to reduce the burden or locally eliminate malaria and other mosquito-borne diseases.” [62] The current mass distribution of LLINs is not sufficient and may not be sustainable. We also need to look to the future, beyond LLINs, for tools.” [63] Insecticide-treated plastic sheeting (ITPS) could be considered among “future prospects for control of malaria and other vector-borne diseases.” [49] The problems of indoor residual spraying in Angola, 13, and the withdrawal of nets observed in villages around Balombo, where more than 50% of nets were torn and discarded within three years, 20 showed the need for new tools, among which could be insecticide-treated plastic sheeting. This induced the comprehensive, long-term, village-scale malaria control program implemented around Balombo town to compare the efficacy of ITPS versus classical LLIN or IRS, alone or in combination. [59] After implementation of vector control the densities of main vectors per CDC Light Trap, installed inside houses, dropped by 72%, infectivity dropped from 4.53%, (n= 375), to 2.73% (n=183), a noteworthy, if not significant, 43% reduction and the inoculation rates decreased similarly by 84%. The four methods had same entomological efficacy. [59] After implementation of vector control the parasite prevalence dropped by 78%, the gametocyte dropped by 76% and the parasite load decreased significantly; an interesting epidemiological output as parasite load is related to malaria morbidity. [64-66] With the four methods it was observed an evolution of parasitological indicators in three steps: first a striking decrease, then a six-year “plateau”, and an important increase due to the national malaria outbreak. During this outbreak, the parasite prevalence was still lower than before vector control but the parasite loads increased. There was also noted a long period without detectable gametocyte (with the technology used). Even if it is known that “a sub-microscopic gametocyte reservoir can sustain malaria transmission” [68] the “low-level gametocytemia corresponds to reduced likelihood of mosquito infection.” [68] The combination of LLIN and ITPS greatly increased the amount of insecticide in the house 59 but did not seem to have produced a particular parasitological advantage compared to LLIN or ITPS alone. This has to be taken into consideration as it was reported that the significant increase in insecticide-based malaria vector control in the past decade has resulted in increasing resistance among malaria vectors because of the selection pressure placed on resistance genes and this could lead to great operational problems. The management of insecticide resistance is of great concern [69], 22-24 Two main types of mechanism have been identified to be involved in insecticide resistance: target-site resistance, due to mutations in the target proteins of insecticides, and metabolic resistance, due to increased detoxification of insecticides. 23 One well known target site resistance is the knockdown resistance (kdr) caused by mutations in the voltage-gated sodium channel gene, which compromises its binding to pyrethroid insecticides. [70] A survey done in 2001 in four sites in the semi-arid coastal provinces of Luanda and Benguela and two sites in Huambo province to determine the Anopheles species present, their sporozoite rates and the frequency of a kdr allele conferring resistance to pyrethroid insecticides reported that « Of 218 An. gambiae (195 M-form and 23 S-form) genotyped for the West African kdr-resistance allele, all were homozygous susceptible ». [71] A study conducted in 2022 at two sentinel sites in the province of Benguela [72] reported « Kdr mutations were surveyed in An. gambiae s.l. The kdr-West L1014F kdr mutation was discovered in both resistant and susceptible An. coluzzii mosquitoes, while the kdr-East L1014S mutation was detected in An. gambiae s.s. for the first time in Benguela Province. No kdr mutations were found in An. arabiensis. An. gambiae s.s. predominantly exhibited the mutant allele L1014F with an allele frequency of 0.90. In total, across both sentinel sites, the overall frequency of 1014F mutation was 0.65, while the 1014S mutation was found to be 0.01. Our study’s novel discovery of the West African kdr-resistance allele 1014F in An. coluzzii and An. gambiae s.s. confirms the presence of pyrethroid resistance in these populations. Interestingly, the first detection to our knowledge of the East African kdr-resistance allele 1014S in An. gambiae s.s. highlights the emergence of this mutation in Benguela Province, showing the importance of continuous monitoring of the setting of insecticide resistances in Anopheles gambiae s.s. populations. This finding suggests an emerging challenge in insecticide resistance, previously unrecorded in this region. The detection of mutations involved in pyrethroid resistance was limited to L1014F and L1014S in An. gambiae s.l. Other potential mechanisms of insecticide resistance, such as metabolic resistance, were not yet explored in Angola. » It is feared that IR could negatively impact the efficacy of pyrethroid treated ITN 25. But the conclusion could be different according to the method of evaluation, laboratory, experimental huts [75-77] or field trial. [78] Conclusions could also be different according to the indicators selected: entomological, immunological, parasitological, epidemiological (see document joined “beware the indicator”). For example, a trial in the village of Kafiné in Côte d’Ivoire, where An. gambiae has a high kdr based resistance to pyrethroids (80%), showed that permethrin treated nets conferred personal protection while no entomological impact was noticed with the method implemented. [79, 80] « In the Department of Korhogo, (Northern Côte d’Ivoire) a longitudinal study was conducted to evaluate the entomologic and epidemiologic impact of nets treated with lambda-cyhalothrin in a region with intense transmission due to An. gambiae highly resistant to pyrethroids with a kdr allelic frequency of around 90%. [81] After installation of ITN it was observed a reduction of the inoculation rate two times more than what naturally reduction which occurred in villages without nets (relative reduction of 52.8%); and the rate of asymptomatic infections was higher in the untreated group than the treated one: 68.5% versus 56.6%, (P < 0>
V. Conclusion
After 11 years of field studies, 136 parasitological cross-sectional surveys, 12,525 thick blood films done on asymptomatic children ≤15-year-old, and microscopically observed, it could be considered that: 1) the four methods of vector control produced similar results in reducing significantly parasite prevalence, parasite load and gametocyte index. 2) After a striking decrease the first year’s post vector control, there was a five to six-year plateau, at a very low level, in the three parasitological indicators. 3) during the malaria outbreak, parasite prevalence increased but was still significantly lower than before vector control, 4) No parasite prevalence rebound was ever noticed, in these field natural conditions, several years after vector control. 5) Malaria outbreak induced an increase of the parasite load, underlining the needs for continuous vector control operations. ITPS may represent an interesting substitute, or complement, to classical LLIN and IRS, especially when, and where, these classical methods cannot be implemented. For example, ITPS can be combined with nets, or house spraying, treated with different insecticides to address the burning issue of insecticide resistance management. The actual community participation in the ITPS installation in their house must be underlined. Therefore, ITPS could be one of the most interesting new available tools to facilitate the targeted elimination of malaria.
Acknowledgements
We thank the Sonamet® Angolese Company Manager and its Medical Department for their permanent support, and the International Sub Sea 7® Company for its important financial support, which made it possible to carry out these studies.
We thank the different B2B MD in charge of this medical service during our study.
We thank the Ministry of Health and the Dr Fortes Chief of the National Malaria Control Program of Angola for his involvement and monitoring of the study.
We thank the Provincial Public Health Department for their appreciated help in field studies and all administrative issues.
Many thanks to V. Foumane who did the training of microscopists, participated in field surveys, thick blood films examination, and did double check with feedback.
Many thanks to agents of MCP: Luis, Almeida, Alcides, who participated in field surveys, and blood films examination.
We thank Mr Timelman who procured the material (treated nets, plastic sheeting) for vector control.
Many thanks also to the communities of the villages who were actually involved in different vector control activities.
Many thanks to teacher John for his English editing.
Funding
The Balombo project was supported by the Sonamet® Angolese Company in the framework of its “Malaria Control Program” managed by its Medical Service; and by the International SubSea 7® Company.
Author’s Contributions
PC designed the protocol, participated to field surveys, analyzed data and wrote the manuscript; JCT participated in field surveys, FM was the head of the Medical Department of the Sonamet Company (Lobito) where all slides were observed and checked; GC was involved in the writing and English version.
Declaration of competing interest
The authors declare that they have no competing interest.
Ethics Statement
« This study was conducted in accordance with the Edinburgh revision of the Helsinki Declaration and was approved by the National Malaria Control Program of the Ministry of Health of Angola, the Ethical authority in charge of approving studies on malaria research in Angola. Written consent (signed by the head of each household) was obtained for all individuals enrolled in the study by the SONAMET Company - Malaria Control Program (MCP) which is responsible for malaria surveillance and control amongst company employees and their families. » Brosseau et al., 2012 The study was done as part, and with, the National Malaria Control Program of Angola, the Benguela Public Health Provincial Delegation and a part of the, in process, Malaria Control Program of the Angolese Sonamet® Company.
References
- World Malaria Report (2024). Addressing inequity in the global malaria response. World Health Organization Geneva.
View at Publisher | View at Google Scholar - Tavares W, Morais J, Martins J et al. (2022). Malaria in Angola: recent progress, challenges and future opportunities using parasite demography studies. Malar J; 21:396.
View at Publisher | View at Google Scholar - (2019). PNCM. Relatório Anual Descritivo da Malária. Programa Nacional de Controle da Malária, Ministério da Saúde de Angola.
View at Publisher | View at Google Scholar - PMI. U.S. (2019). President’s Malaria Initiative Angola Malaria Operational Plan 2020. Washington DC: United States Agency for International Development (USAID).
View at Publisher | View at Google Scholar - Plucinski MM, Ferreira M, Ferreira CM et al. (2017). Evaluating malaria case management at public health facilities in two provinces in Angola. Malar J; 16:186.
View at Publisher | View at Google Scholar - Fançony C, Brito M, Gil JP. (2016). 4 Plasmodium falciparum drug resistance in Angola. Malar J; 15:74.
View at Publisher | View at Google Scholar - Foumane Ngane V, Allico Djaman J, Culeux C et al. (2015). Molecular epidemiology of drug-resistant Plasmodium falciparum in Benguela province, Angola. Malar J; 14:1134.
View at Publisher | View at Google Scholar - Fortes F, Dimbu R, Figueiredo P et al. (2011). Evaluation of prevalence's of pfdhfr and pfdhps mutations in Angola. Malar J; 10:22.
View at Publisher | View at Google Scholar - Fortes F. (2011). Perfl epidemiológico das principais doenças parasitárias endémicas em Angola. Doctoral Thesis, Universidade NOVA de Lisboa, Instituto de Higiene e Medicina Tropical.
View at Publisher | View at Google Scholar - Guthmann JP, Ampuero J, Fortes F et al. (2005). Antimalarial efficacy of chloroquine, amodiaquine, sulfadoxine-pyrimethamine, and the combinations of amodiaquine + artesunate and sulfadoxine-pyrimethamine + artesunate in Huambo and Bie provinces, central Angola. Trans R Soc Trop Med Hyg; 99:485–492.
View at Publisher | View at Google Scholar - Plucinski MM, Dimbu PR, Macaia AP et al. Efficacy of artemether-lumefantrine, artesunate-amodiaquine, and dihydroartemisinin-piperaquine for treatment of uncomplicated Plasmodium falciparum malaria in Angola, 2015. Malar J 2017; 16:62.
View at Publisher | View at Google Scholar - Davlantes E, Dimbu PR, Ferreira CM et al. (2018). Efficacy and safety of artemether-lumefantrine, artesunate-amodiaquine, and dihydroartemisinin-piperaquine for the treatment of uncomplicated Plasmodium falciparum malaria in three provinces in Angola, 2017. Malar J; 17:144.
View at Publisher | View at Google Scholar - Somandjinga M, Lluberas M, Jobin W. (2009). Difficulties in organizing first indoor spray programme against malaria in Angola under the President's Malaria Initiative. Bull Wld Hlth Org; 87(11):871-874.
View at Publisher | View at Google Scholar - PMI. U.S. (2021). President’s Malaria Initiative Angola Malaria Operational Plan FY 2022. Washington, DC: United States Agency for International Development (USAID).
View at Publisher | View at Google Scholar - PMI. U.S. (2020). President’s Malaria Initiative Angola Malaria Operational Plan FY 2021. Washington DC: United States Agency for International Development (USAID).
View at Publisher | View at Google Scholar - Morais J, Franscisco M, de Vasconcelos JN et al. (2019). Epidemiological baseline cross-sectional study to monitor P. falciparum transmission intensity in Southern Angola. Luanda, Angola: INIS, CISA, Angolan NMCP, Elimination 8, UCSF, Global Fund; 49.
View at Publisher | View at Google Scholar - Eisele T., Thwing J., Keating J. Claims about the misuse of insecticide-treated mosquito nets: are these evidence-based? PLoS Med 2011;8(4): e1001019
View at Publisher | View at Google Scholar - McLean K, Byanaku A, Kubikonse A et al. Fishing with bed-nets on Lake Tanganyika: a randomized survey. Malar J 2014; 13:395.
View at Publisher | View at Google Scholar - Kibe L., Kamau A., Gachigi J., Habluetzel A., Mbogo C. A formative study of disposal and re-use of old mosquito nets by communities in Malindi, Kenya. Malaria World J 2019; 3:6–9.
View at Publisher | View at Google Scholar - Carnevale P., Toto J.C., Foumane V et al. Co-evolution of the presence of long-lasting insecticide treated nets and Plasmodium falciparum Welch, 1897 prevalence in Cahata village (Benguela Province, Angola) during a village scale long-term of malaria vector control program. Asian J Res Inf Dis 2021; 7(4):21–32.
View at Publisher | View at Google Scholar - Monroe A, Moore S, Olapeju B et al. Unlocking the human factor to increase effectiveness and sustainability of malaria vector control. Malar J 2021; 20(1):404.
View at Publisher | View at Google Scholar - Hemingway J, Ranson H, Magill A et al. Averting a malaria disaster: will insecticide resistance derail malaria control? Lancet 2016; 387(10029):1785-1788.
View at Publisher | View at Google Scholar - Hemingway J, Ranson H. Insecticide resistance in insect vectors of human disease. Annu Rev Entomol 2000; 45:371-391.
View at Publisher | View at Google Scholar - Ranson H, Lissende N. Insecticide resistance in African anopheles mosquitoes: a worsening situation that needs urgent action to maintain malaria control. Trends Parasitol 2016; 32:187–196.
View at Publisher | View at Google Scholar - N'Guessan R, Corbel V, Akogbeto M, Rowland M. Reduced efficacy of insecticide-treated nets and indoor residual spraying for malaria control in pyrethroid resistance area, Benin. Emerg Infect Dis 2007; 13(2):199-206.
View at Publisher | View at Google Scholar - Kleinschmidt I, Mnzava A, Kafy H et al. Design of a study to determine the impact of insecticide resistance on malaria vector control: a multi-country investigation. Malar J 2015; 14:282.
View at Publisher | View at Google Scholar - Kleinschmidt I, Schwabe C, Shiva M et al. Combining indoor residual spraying and insecticide-treated net interventions? Am J Trop Med Hyg 2009; 81 (3); 519-524.
View at Publisher | View at Google Scholar - Protopopoff N, Wright A, West P et al. Combination of Insecticide Treated Nets and Indoor Residual Spraying in Northern Tanzania Provides Additional Reduction in Vector Population Density and Malaria Transmission Rates Compared to Insecticide Treated Nets Alone: A Randomized Control Trial. PLoS One 2015; 10(11): e0142671.
View at Publisher | View at Google Scholar - Guillet P, N'Guessan R, Darriet F et al. Combined pyrethroid and carbamate 'two-in-one' treated mosquito nets: field efficacy against pyrethroid-resistant Anopheles gambiae and Culex quinquefasciatus. Med Vet Entomol 2001; 15(1):105-112.
View at Publisher | View at Google Scholar - Pennetier C, Bouraima A, Chandre F et al. Efficacy of Olyset® Plus, a new long-lasting insecticidal net incorporating permethrin and piperonyl-butoxide against multi-resistant malaria vectors. PLoS One 2013 ; 8(10) : e75134.
View at Publisher | View at Google Scholar - Protopopoff N, Mosha J, Lukole E et al. Effectiveness of a long-lasting piperonyl butoxide-treated insecticidal net and indoor residual spraying interventions, separately and together, against malaria transmitted by pyrethroid-resistant mosquitoes: a cluster randomized controlled, two-by-two factorial design trial. Lancet 2018; 391(10130):1577-1588.
View at Publisher | View at Google Scholar - Tungu P, Waweru J, Karthi S, Wangai J, Kweka E. Field evaluation of Veralin® an alpha-cypermethrin + PBO long-lasting insecticidal net, against natural populations of Anopheles funestus in experimental huts in Muheza, Tanzania. Curr Res Parasitol Vector Borne Dis 2021 ; 1 :100030.
View at Publisher | View at Google Scholar - Martin J, Mosha F, Lukole E et al. Personal protection with PBO-pyrethroid synergist-treated nets after 2 years of household use against pyrethroid-resistant Anopheles in Tanzania. Parasit Vectors 2021 ; 14(1) :150.
View at Publisher | View at Google Scholar - Roh M, Oundo B, Dorsey G et al. A quasi-experimental study estimating the impact of long-lasting insecticidal nets with and without piperonyl butoxide on pregnancy outcomes. Malar J 2022; 21(1):5.
View at Publisher | View at Google Scholar - Mechan F, Katureebe A, Tuhaise V et al. LLIN evaluation in Uganda project (LLINEUP): The fabric integrity, chemical content and bio efficacy of long-lasting insecticidal nets treated with and without piperonyl butoxide across two years of operational use in Uganda. Curr Res Parasitol Vector Borne Dis 2022; 2(100092).
View at Publisher | View at Google Scholar - Djènontin A, Ahoua Alou L, Koffi A et al. Insecticidal and sterilizing effect of Olyset Duo®, a permethrin and pyriproxyfen mixture net against pyrethroid-susceptible and-resistant strains of Anopheles gambiae s.s.: a release-recapture assay in experimental huts. Parasite Vectors 2015 ;22 :27.
View at Publisher | View at Google Scholar - Sagnon N, Pinder M, Tchicaya E et al. To assess whether addition of pyriproxyfen to long-lasting insecticidal mosquito nets increases their durability compared to standard long-lasting insecticidal mosquito nets: study protocol for a randomized controlled trial. Trials 2015; 16:195.
View at Publisher | View at Google Scholar - Tiono A, Pinder M, N'Fale S et al. The AvecNet® Trial to assess whether addition of pyriproxyfen, an insect juvenile hormone mimic, to long-lasting insecticidal mosquito nets provides additional protection against clinical malaria over current best practice in an area with pyrethroid-resistant vectors in rural Burkina Faso: study protocol for a randomized controlled trial. Trials 2015; 16:113.
View at Publisher | View at Google Scholar - Tiono A, Ouédraogo A, Ouattara D et al. Efficacy of Olyset Duo® a bednet containing pyriproxyfen and permethrin, versus a permethrin-only net against clinical malaria in an area with highly pyrethroid-resistant vectors in rural Burkina Faso: a cluster-randomized controlled trial. Lancet 2018; 392(10147):569-580.
View at Publisher | View at Google Scholar - Toé K, Mechan F, Tangena J et al. Assessing the impact of the addition of pyriproxyfen on the durability of permethrin-treated bed nets in Burkina Faso: a compound-randomized controlled trial. Malar J 2019; 18(1):383.
View at Publisher | View at Google Scholar - Ngufor C, N'Guessan R, Boko P et al. Combining indoor residual spraying with chlorfenapyr and long-lasting insecticidal bed nets for improved control of pyrethroid-resistant Anopheles gambiae: an experimental hut trial in Benin. Malar J 2011;10:343
View at Publisher | View at Google Scholar - Accrombessi M, Cook J, Dangbenon E et al. Efficacy of pyriproxyfen-pyrethroid long-lasting insecticidal nets (LLINs) and chlorfenapyr-pyrethroid LLINs compared with pyrethroid-only LLINs for malaria control in Benin: a cluster-randomised, superiority trial. Lancet 2023;401(10375):435-446.
View at Publisher | View at Google Scholar - Zahouli JZB, Edi CAV, Yao LA et al. Small-scale field evaluation of PermaNet® Dual (a long-lasting net coated with a mixture of chlorfenapyr and deltamethrin) against pyrethroid-resistant Anopheles gambiae mosquitoes from Tiassale, Cote d'Ivoire. Malar J 2023; 22(1):36.
View at Publisher | View at Google Scholar - Accrombessi M, Cook J, Dangbenon E et al. Effectiveness of pyriproxyfen-pyrethroid and chlorfenapyr-pyrethroid long-lasting insecticidal nets (LLINs) compared with pyrethroid-only LLINs for malaria control in the third-year post-distribution: a secondary analysis of a cluster-randomised controlled trial in Benin. Lancet Infect Dis 2024; 24(6):619-628.
View at Publisher | View at Google Scholar - Sovi A, Yovogan B, Adoha CJ et al. Efficacy of pyrethroid-pyriproxyfen and pyrethroid-chlorfenapyr nets on entomological indicators of malaria transmission: third year of a randomised controlled trial in Benin. Sci Rep 2024; 14(1):12958.
View at Publisher | View at Google Scholar - Yovogan B, Sovi A, Djènontin A et al. The impact of pyrethroid-pyriproxyfen and pyrethroid-chlorfenapyr long-lasting insecticidal nets on density of primary malaria vectors Anopheles gambiae s.s. and Anopheles coluzzii in Benin: a secondary analysis of a cluster randomized controlled trial. Parasite Vectors 2024; 17(1):7.
View at Publisher | View at Google Scholar - Burns M. Evaluating insecticide-treated polyethylene sheeting for malaria control in complex emergencies: an intersectoral approach. Humanitarian Exchange 2005 ; 31 :14-16.
View at Publisher | View at Google Scholar - Diabate A, Chandre F, Rowland M et al. The indoor use of plastic sheeting pre-impregnated with insecticide for control of malaria vectors. Trop Med Int Hlth 2006; 11(5):597-603.
View at Publisher | View at Google Scholar - Messenger L, Miller N, Adeogun A et al. The development of insecticide-treated durable wall lining for malaria control: insights from rural and urban populations in Angola and Nigeria. Malar J 2012; 18(11):332.
View at Publisher | View at Google Scholar - Chandre F, Dabire R, Hougard JM et al. Field efficacy of pyrethroid treated plastic sheeting (durable lining) in combination with long-lasting insecticidal nets against malaria vectors. Parasite Vectors 2010; 3(1):65.
View at Publisher | View at Google Scholar - Djènontin A, Chandre F, Dabiré K et al. Indoor use of plastic sheeting impregnated with carbamate combined with long-lasting insecticidal mosquito nets for the control of pyrethroid-resistant malaria vectors. Am J Trop Med Hyg 2010; 83(2):266-270.
View at Publisher | View at Google Scholar - Djenontin A, Chabi J, Baldet T et al. Managing insecticide resistance in malaria vectors by combining carbamate-treated plastic wall sheeting and pyrethroid-treated bed nets. Malar J 2009; 8:233.
View at Publisher | View at Google Scholar - Ngufor C, Chouaïbou M, Tchicaya E et al. Combining organophosphate-treated wall linings and long-lasting insecticidal nets fails to provide additional control over long-lasting insecticidal nets alone against multiple insecticide-resistant Anopheles gambiae in Côte d'Ivoire: an experimental hut trial. Malar J 2014 ;13 :396
View at Publisher | View at Google Scholar - Kleinschmidt I, Schwabe C, Shiva M et al. Combining indoor residual spraying and insecticide-treated net interventions. Am J Trop Med Hyg 2009; 81:519–524.
View at Publisher | View at Google Scholar - Okumu FO, Mbeyela E, Lingamba G et al. Comparative field evaluation of combinations of long-lasting insecticide treated nets and indoor residual spraying, relative to either method alone, for malaria prevention in an area where the main vector is Anopheles arabiensis. Parasite Vectors 2013; 6:46.
View at Publisher | View at Google Scholar - Messenger L, Matias A, Manana et al. Multicentre studies of insecticide-treated durable wall lining in Africa and South-East Asia: entomological efficacy and household acceptability during one year of field use. Malar J 2012; 11:358.
View at Publisher | View at Google Scholar - Messenger L, Larsen M, Thomas J, Rowland M. Installation of insecticide-treated durable wall lining: evaluation of attachment materials and product durability under field conditions. Parasite Vectors 2014; 7:508.
View at Publisher | View at Google Scholar - Brosseau L, Drame P, Besnard P et al. Human antibody response to Anopheles saliva for comparing the efficacy of three malaria vector control methods in Balombo, Angola. PLoS One 2012; 7(9): e44189.
View at Publisher | View at Google Scholar - Carnevale P, Toto JC, Foumane V et al. The Balombo Project (Angola). A long-term village-scale malaria vector control program, comparing four methods: long-lasting insecticide-treated nets alone, insecticide-treated plastic sheeting alone or combined with long-lasting insecticide-treated nets, or following two rounds of indoor residual spraying. I. First entomological and parasitological evaluation. Clinical Reviews and Case Reports 2024; 3(6).
View at Publisher | View at Google Scholar - García GA, Hergott DEB, Phiri WP, Perry M, Smith J, et al. Mapping and enumerating houses and households to support malaria control interventions on Bioko Island. Malar J. 2019 22;18(1):283.
View at Publisher | View at Google Scholar - Soares Magalhães R, Langa A, Sousa-Figueiredo JC, Clements A, Vaz Nery S. Finding malaria hot-spots in northern Angola: the role of individual, household and environmental factors within a meso-endemic area. Malaria J 2012, 11 :385.
View at Publisher | View at Google Scholar - Benelli G, Beier J. Current vector control challenges in the fight against malaria. Acta Trop 2017; 174:91-96.
View at Publisher | View at Google Scholar - Macdonald M. Long-Lasting Insecticidal Nets for Malaria Control in Myanmar and Nigeria: Lessons From the Past, Tools for the Future. Glob Hlth Sci Pract 2018; 6(2):237-241.
View at Publisher | View at Google Scholar - Bouvier P, Rougemont A, Breslow N et al. Seasonality and malaria in a West African village: does high parasite density predict fever incidence? Am J Epidemiol. 1997; 145(9):850-857.
View at Publisher | View at Google Scholar - Rogier C, Commenges D, Trape J. Evidence of an age dependent pyrogenic threshold of Plasmodium falciparum parasitaemia in highly endemic populations. Am J Trop Med Hyg 1996; 54(6):613–619.
View at Publisher | View at Google Scholar - Rogier C, Henry MC, Spiegel A. Diagnostic des accès palustres en zone d’endémie : bases théoriques et implications pratiques. Méd Trop 2001; 61:27-46.
View at Publisher | View at Google Scholar - Rogier C, Fusai T, Pradines B, Trape J-F. Comment évaluer la morbidité attribuable au paludisme en zone d'endémie ? Rev Epidém Santé Publique 2005; 53:299-309.
View at Publisher | View at Google Scholar - Karl S, Gurarie D, Zimmerman P et al. A sub-microscopic gametocyte reservoir can sustain malaria transmission. PLoS One 2011; 6(6): e20805.
View at Publisher | View at Google Scholar - World Health Organization GMP. Global plan for Insecticide Resistance Management in malaria vectors (GPIRM). WHO Library Cataloguing-in-Publication Data 2012.
View at Publisher | View at Google Scholar - Martinez-Torres D, Chandre F, Williamson MS et al. Molecular characterization of pyrethroid knockdown resistance (kdr) in the major malaria vector Anopheles gambiae s.s. Insect Mol Biol 1998; 7:179–184.
View at Publisher | View at Google Scholar - Cuamba N, Kwang SC, Townson H. Malaria vectors in Angola: distribution of species and molecular forms of the Anopheles gambiae complex, their pyrethroid insecticide knockdown resistance (kdr) status and Plasmodium falciparum sporozoite rates. Malar J 2006; 5:1–6.
View at Publisher | View at Google Scholar - Alves G, Troco A, Seixas G, et al. Molecular and entomological surveillance of malaria vectors in urban and rural communities of Benguela Province, Angola. Parasite Vectors 2024; 17:112
View at Publisher | View at Google Scholar - Kleinschmidt I, Bradley J, Knox T et al. Implications of insecticide resistance for malaria vector control with long-lasting insecticidal nets: a WHO-coordinated, prospective, international, observational cohort study. Lancet Infect Dis. 2018; 18(6): 640–649.
View at Publisher | View at Google Scholar - Messenger LA, Rowland M. Insecticide-treated durable wall lining (ITWL): future prospects for control of malaria and other vector-borne diseases. Malar J 2017; 16(1):213.
View at Publisher | View at Google Scholar - Darriet F, Guillet P, N’Guessan R et al. 1999. The impact of permethrin and deltamethrin resistance in Anopheles gambiae s.s. on the efficacy of insecticide-treated mosquito nets. Documents WHO/VBC/99.1002, WHO/MAL/99.1088
View at Publisher | View at Google Scholar - Asidi AN, N’Guessan R, Hutchinson RA et al. 2004. Experimental hut comparisons of nets treated with carbamate or pyrethroid insecticides, washed or unwashed, against pyrethroid-resistant mosquitoes. Med Vet Entomol 18: 134–140.
View at Publisher | View at Google Scholar - Koffi A, Aloul A, Djenontin A, Kabran JP et al. Efficacy of Olyset Duo®, a permethrin and pyriproxyfen mixture net against wild pyrethroid-resistant Anopheles gambiae s.s. from Côte d’Ivoire: an experimental hut trial. Parasite 2015; 22, 28.
View at Publisher | View at Google Scholar - Rehman AM, Mann AG, Schwabe C et al. Five years of malaria control in the continental region, Equatorial Guinea. Malar J 2013;12:154.
View at Publisher | View at Google Scholar - Doannio J, Dossou-Yovo J, Diarrassouba S et al. Efficacité des moustiquaires pré-imprégnées de perméthrine Olyset Net® en zone de résistance des vecteurs aux pyréthrinoïdes. I. Evaluation entomologique. Med Trop 1999 ; 59, 349-354.
View at Publisher | View at Google Scholar - Henry M-C, Doannio JMC, Darriet F et al. Efficacité des moustiquaires pré-imprégnées de perméthrine Olyset Net® en zone de résistance des vecteurs aux pyréthrinoïdes. II. Evaluation parasito-clinique. Med Trop 1999 ; 59 :355–357.
View at Publisher | View at Google Scholar - Henry MC, Assi SB, Rogier C et al. Protective efficacy of lambda-cyhalothrin treated nets in Anopheles gambiae pyrethroid resistance areas of Côte d’Ivoire. Am J Trop Med Hyg, 2005; 73(5): 859–964.
View at Publisher | View at Google Scholar - Kleinschmidt I, Bradley J, Knox TB et al. Implications of insecticide resistance for malaria vector control with long-lasting insecticidal nets: a WHO-coordinated, prospective, international, observational cohort study. Lancet Infect Dis 2018;18(6):640-649.
View at Publisher | View at Google Scholar - Messenger L, Rowland M. Insecticide-treated durable wall lining (ITWL): future prospects for control of malaria and other vector-borne diseases. Malar J 2017; 16(1):213.
View at Publisher | View at Google Scholar
