

Research Article | DOI: https://doi.org/10.31579/2835-8147/038
Empowering Nurse-CHO’s to be an effective Mid-Level Health Provider
Research Scholar. Department of Management, Brainware University, Barasat, Kolkata.
*Corresponding Author: Suresh Kishanrao, MD, DIH, DF, FIAP, FIPHA, FISCD, Family Physician & Public Health Consultant, Bengaluru, India
Citation: K Suresh (2023), Empowering Nurse-CHO’s to be an effective Mid-Level Health Provider! Clinics in Nursing, 2(5); DOI:10.31579/2835-8147/038
Copyright: © 2023, K Suresh. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 13 October 2023 | Accepted: 23 October 2023 | Published: 03 November 2023
Keywords: proportion persons responded as ailing (ppra); national health mission (nhm); primary health centre (phc); health & wellness centres (hwc-subcentre level); community health officers (chos)
Abstract
Nurses have played a pivotal role in Indian health care system. The Bhore committee report in mid-1940’s, envisaged a strong need for providing newer roles for nurses in some far flung rural, tribal, Hilly, and even urban poor populations, where doctors may not be available. Taking cognisance of non-availability of trained manpower and doctors even in some of the primary health centres, the Government of India (GOI), National Health Mission (NHM) has created a new category of community health officer (CHO) with its constructed roles and responsibilities for public health. According to NMC bill 2019, nurses are the first choice for CHO, and this will also pave the way for professional development. Though Community health nursing is integrated in the curriculum of GNM and BSc Nursing courses, but their exposure to community health nursing, midwifery and sickness care is limited. To compensate this limitation, GOI has initiated a bridge course titled” Bridge Programme of Certificate in Community Health for Nurses (BPCCHN) to update the knowledge and skills of working nurses in public sector in 2017.National Sampl Surveys Organizations (NSSO) 75th (2017-18) reported proportion of persons that responded as ailing (PPRA) was 7.5% of the (9.1% among urban and 6.8% among rural) population during last 15-day reference period of the survey. Therefore, sickness care is a key intervention under UHC. While private sector provides care to 70% of outpatient episodes of the population, the apathy of public doctors leads to unregulated private practitioners in health sector, in Rural area. The Primary care places a greater emphasis on the health of the whole person rather than a specific organ or system, contributing to reduction in mortality rates due to comprehensive continuous and accumulated care.
Materials & Methods:
This article is an effort to share the experience of first five years (2018-23). Thirty-five (25 R & 10 U) SCHWCs in Karnataka, Maharashtra, Tamil Nadu, Kerala, Andhra Pradesh, Madhya Pradesh, and Utter Pradesh were visited as a consultant for various program reviews and therefore may not be representative but do indicate challenges of CHOs and allow stakeholders to plan appropriate support them. Observations of CHO’s task performance in general, and some expanded tasks like diagnosis and treatment of cases beyond minor ailments, common ENT, Oral and Eye conditions, screening for mental health disturbances and emergency medical services. Male CHO’s contributions in MCH services (except immunizations) and deliveries both at centre & homes have not added value.
Introduction
Nurses have played a pivotal role in Indian health care system. The Bhore committee report in mid-1940’s, envisaged a strong felt need
for providing newer roles for nurses in some far flung rural, tribal, Hilly, and even urban poor populations [1]. NHM was launched by the government of India in 2013 subsuming the National Rural Health Mission (Launched in 2005) and the National Urban Health Mission (Launched in 2013). 150,000 of our basic health infra-structure of sub-centres and minimum need PHCs catering for a population of 5000 in the plain, and 3000 population in hilly, tribal areas were upgraded and renamed "Health and Wellness centres" under National Health Mission in 2018. They are expected to provide comprehensive primary health care including running daily 6 hours of OPD for Providing universal health care (UHC) to treat as many ailments as possible. A community Health Officer’s post is created and trained nurses or Ayurvedic doctors are being posted to complement the existing staffing of a male and female health worker implementing the national health programmes and running daily outpatient care for 6 hours a day in addition to running MCH clinics for ANC, Immunization etc and minor ailments (for only few days a week) hitherto since mid-1970’s under Multipurpose worker’s scheme.
Taking cognisance of non-availability of trained manpower and doctors even in some of the primary health centres, the Government of India initiated a bridge course to update knowledge and skills of graduate nurses and Ayurvedic doctors. The course is being funded by MOHFW, Govt. of India and the desiring nurses are selected based on selection test, aptitude for working in rural area. The course is run for 6 months with skill development at the district hospital level. They are taught clinical skills, basics of filed epidemiology of communicable, non- communicable diseases, classification of sicknesses (based on IMNCI experience since 1995) based on logarithmic flow charts identification, and management of common health problems and provide referrals to cases of serious illnesses or case they can’t manage at local level to higher health facility besides health promotion activities.
This initiative aimed to provide a greater role to the nursing profession and boost the health care delivery in the rural and far-flung rural, tribal, Hilly and Urban Poor populations. Their preservice bridge course is aimed to:
- Enhance knowledge & skills of learners in providing community health care services.
- Develop competencies in dealing with issues of public health.
- Provide comprehensive primary care based on protocols appropriate at PHC level.
- Perform preventive and promotive actions for improving community health.
- Perform common laboratory investigations.
- Provide treatment based on protocols as appropriate to subcentre level.
This article is an effort to share the experience of first five years (2018-23) of about 35 H&WCs across the country (R=25, U=10) mainly in Karnataka complimented by anecdotes from other states the author has observed as a PH consultant in various program reviews in 2022 and 2023. The sample is not representative, but observations hold good for most units if not all SC level H&WCs across the country.
Public Health Nursing has undergone many changes in Public Health a responsibility of National and Provincial Governments in India has a long history. Let me recount them before I discuss the current challenge.
1. Midwives Era (MWE):
India had well-trained European and indigenous midwives during the time of British rule. As early 1854 the British Government sanctioned the opening of the first formal training school for midwives followed by 8 more across the country. These midwifery schools had trained midwives from Britain and indigenous midwives as faculty. These midwives were skilled to practice childbirth care independently. During the 19thCentury, there were plenty of trained midwives, but no nurses were available to care for the sick and injured. To overcome this shortage of nurses, the then surgeon general of the Madras Presidency trained such midwives for six months in nursing. Those who succeeded in both contents were given Nurse and midwifery certificate as midwifery required more skills than ‘sick nursing and those who did not qualify as midwives were given a certificate in ‘sick nursing’. The strong midwifery profession lost its importance after independence for various reasons. The dilution in the midwifery profession, is attributed to amended regulations, lack of social or political priorities, and change in health programme directions from maternal health to Family planning and later family welfare [2].
2. Auxiliary Nurse Midwife Era (ANME):
Acute shortage of nurses to manage injuries in the Second World War (1939–1945), the British Government had initiated a six-month course for intensive training in nursing and midwifery, which led to the formation of the Auxiliary Nursing and Midwifery Service in 1942. After the War, to continue in the government service, the newly created cadres of auxiliary nurses had to undergo one and half years of training in midwifery to get their certification as midwives thus making the total duration of training of 2 years. In earlier part of the 19th Century ‘Zanana hospitals’ for women in smaller towns for birthing largely run by nurses and midwives due to shortage of qualified female doctors and the reluctance of women to be attended by male doctors. In Independent India, the midwives were trained for a period of 2 years out of which, minimum 6 months were exclusively dedicated in labour room to acquire the requisite skill of conducting normal delivery, identifying obstructed labour and referral. Nursing and midwifery have been regarded as low-value professions to provide support to doctors, not as independent practitioners of midwifery [2]
3. Multipurpose Health worker- female Era (MPWE):
Until the early 1970s, ANMs were providing maternal and child health care, including domiciliary birthing in rural areas. In 1974, MPHW (Male/female) Scheme was launched for the delivery of preventive and promotive health care services to the community at the level of Sub-Health Centres (SHCs), the most peripheral health facilities, covering 5000 population in plains and 3000 population in hilly. It mainly focused on disease control programs, detection and control of epidemic outbreaks, environmental sanitation, safe drinking water, first aid in emergencies like accidents, injuries, burns etc. ANMs were designated as multipurpose workers (MPW-F) to provide care for multiple national programs along with MCH services as enlisted above.[3]. With the launch of MPW health workers, ANM’s basic training was reduced from 24 months to 18 months with a reduction of time exposed for the midwifery component. This further deskilled the midwifery role and emphasized community nursing and primary health-care role [6].
Promotion of Institutional Child birthing- an Onslaught on midwifery?
Instead of strengthening midwifery training, cadre and services, the Government of India, under National Rural Health Mission (NRHM), developed a policy of promoting ‘institutional childbirth’ by providing cash incentives to mothers. This ‘Janani Suraksha Yojana’ is supporting large-scale development of village-level health volunteers called Accredited Social Health Activists (ASHA). They also introduced a short training course of skilled birth attendance, for MPW-F and GNM certificate holding staff nurses to build midwifery skills to attend to women who would not go to institutions for various reasons. Due to these changes, the priority of ANMs and the public health system shifted from birth care to all national health programmes. Whereas today’s Female health workers are doing a good job of tasks of antenatal care (ANC), Immunization, disease surveillance, vector borne diseases, family planning motivation and minor ailments treatments on 2-3days a week, the same is not true when it comes to skilled birth attendance, postnatal care, home based new born care (HNBC), non-communicable diseases (hypertension, diabetes, cervical and other cancers) screening, running regular out patients for 6 hours as envisaged in NHP 2017.
1. Lady Health Visitors (Senior Health Assistant- Female):
To contain the emerging dissatisfaction in health services, particularly on job supervision and guidance of MPW (F) rural areas, the GOI introduced the Minimum Needs Programme (MNP) in the Fifth Five Year Plan (1974), that recruited young women as LHV s providing pre-service training for 2 years along with in service training of 6 months for in-service ANMs based on seniority to compliment the supervisory role. The effort was short lived for 5 years, as a result the supervisory tire continued to be the weakest link even today [2].
During the 5th five-year plan (1974-79) Fresh Class 12 passed candidates were directly recruited (50%) and provided in-service training for 2 years. These were some young ladies who were with better educational and intellectual capabilities, the supervisory work was getting due attention. Unfortunately, these courses were abruptly stopped, and the country continued the promotional ANMs cadre with 6 months training.
2. GNM in Health System:
Under the MNP, trained GNMs were recruited and posted in upgraded 24X7 PHCs and other institutions at town level to ensure the client & families to receive the best treatment and care, provide direct patient care, monitor patients' vital signs and coordinate with other members of the healthcare team for health and family welfare services mobilization.
3. District Public Health Nurses (DPHNE):
The District Public Health Nurses (DPHNs) are class III employees, originally from Maternal and Child Health division of Department of health. They are primarily responsible for monitoring maternal and child health services in the district. Some of the sates have created a gazetted post of District Public Health Nursing Officers (DPHNOs) Gazetted officers’ class II under the Family Planning wing. They were primarily The DPHNs based on their seniority were promoted and were responsible for supervising the family planning activities in the district. Over the years, both have come to have the same job profile.
4. Graduate Nurses and Community Health Officers (CHO):
The National Health Policy (NHP, 2002 and 2017) laid emphasis on improving the skill-level of nurses and on increasing the ratio of degree-holding nurses vis-à-vis diploma-holding nurses in the health system. Until recently Graduates nurses were appointed only in Hospital services. Community health nursing is integrated in the curriculum of GNM and BSc Nursing courses but their exposure to community health nursing, midwifery and sickness care is limited. National Health Mission (NHM) has declared a new pivotal role of community health officer (CHO) with its constructed roles and responsibilities for public health. According to NMC bill 2019, nurses are the first choice for CHO, and this will also pave the way for professional development. The Government of India has initiated a bridge course to update the knowledge and skills of working nurses (having a qualification of General Nurse Midwifery) or fresh nursing graduates only in 2017. Titled as” Bridge Programme of Certificate in Community Health for Nurses (BPCCHN). The desiring nurses are selected based on selection test, aptitude for working in rural area. The course is run for 6 months with skill development at the district hospital level. They are taught clinical skills, basic epidemiology of communicable, non- communicable diseases, identification, basic management of common health problems and provide referral in case of serious illnesses to higher health facility besides health promotion activities. Once the course is completed after passing a final examination, they are placed in the health and wellness centres. This initiative is supposed to provide a greater role to the nursing profession and boost the health care delivery in the rural and far-flung rural India. As midlevel health care provider they will reduce the burden of other healthcare professionals and contribute to achieve the aim of Universal Health Care by 2030 [7]. While the eligibility for CHO includes graduates in Ayurvedic Medicine (BAMS) and B.Sc. (Nursing), given the syllabus of Nursing not promoting early diagnosis and treatment, the initial experiences indicate certain challenges. This article does a SWOT analysis of the preparedness of the Nurses to fulfil the role of CHOs and advocates for necessary support by the Health and Family Welfare department, District Hospitals conducting the Bridge course and Nursing Education to review the syllabus to cover the missing skills.
Burden of Sickness in India:
National Sampl Surveys Organizations (NSSO) 75th (2017-18) reported proportion of persons that responded as ailing (PPRA) was 7.5% of the (9.1% among urban and 6.8% among rural) population during last 15-day reference period of the survey [6]. Gender wise PPRA indicated the proportion to be around 6.7% male in and in female-8.3%. Age specific ailment reporting was highest of 27.7% among persons aged 60 years and above followed 11.4% among 40-59 years, 8.5% among under-fives, 5.4% among 20-39, 4.8% among 5-14 years and least among 15-29 aged-3.3%. Similar trend was observed among both genders.
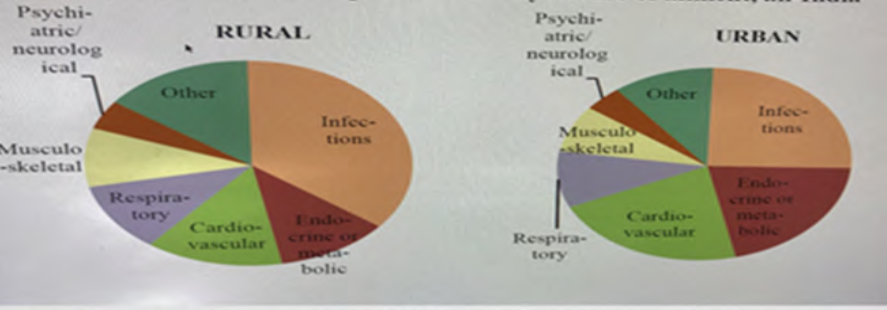
Figure 1: Broad category of illnesses
Broad category of illnesses (Figure 1) indicates that both in Urban (35.7%) and rural (25.4%) area infections were dominant, followed by cardiovascular diseases. While metabolic disease in urban areas were almost double compared to rural area. It is also evident that the proportion of CVDs and Metabolic diseases was significantly higher in urban areas [8]. The first Health and Wellness Centre (HWC) under Ayushman Bharat was inaugurated by the Prime Minister Shri Narendra Modi at Jangla in Bijapur Chhattisgarh, on 14thApril 2018.
The revised IPHS 2022 guidelines classify the HWCs as:
1. Health and Wellness Centres - Primary Health Centre:
- HWC-PHC in rural areas
- HWC- UPHC in urban areas
2. Health and Wellness Centres - Sub Health Centre:
- Health and Wellness Centre - Sub Health Centre in rural areas
- Urban Health & Wellness Centre in urban areas
- Population Norm for HWC-SHC (rural): In rural areas, one Sub Health Centre is established for every 5000 population in plain areas and 3000 population in hilly/tribal/desert areas.
- UHWC (urban): In urban areas one Urban-HWC per 15,000-20,000 population caters predominantly to poor and vulnerable populations, residing in slums or other such pockets.
Discussions
For the first time in Indian Public Health history NHP 2017 committed for providing at least 6 hours OPD daily for case management in 150,000 Health and Wellness Centres (HWCs) across the country. The HWC at the Sub Health Centre level is equipped and staffed by a trained Primary Health Care team, comprising of multi-Purpose Workers (male and female) & ASHAs and led by a Mid-Level Health Provider (MLHP), to deliver an expanded range of services. A CHO {Mid-level Health Care Provider (MLHP)} is the first point of care or source of information for the health- related issues for the community by the virtue of the proximity of HWCs to its catchment population. S/he will provide OPD services with the support existing Male and Female Health workers.
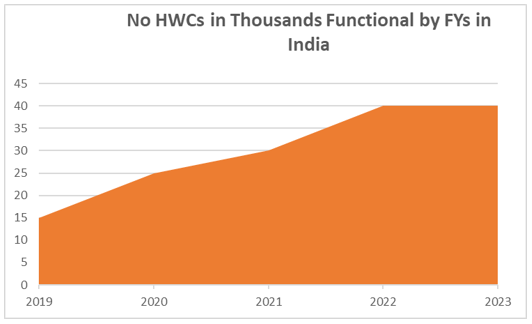
Over the last 5 years all the SC level Health and Welfare Centres have been claimed to be established and their expansion by the year is shown in the graph above.
These centres are expected to deliver Comprehensive Primary Health Care (CPHC) bringing healthcare closer to the homes of people covering both maternal and child health services and non-communicable diseases, including free essential drugs and diagnostic services. The general status is summarised before discussing the value-add of the CHOs based on Primary Sources & Field Observations as of 30 September 2023:
- All the states claim having established upgrading HSC s & PHCs to HWCs
- One thirds of the states felt that converting HSCs into HWC’s in metropolitan cities is non-viable for want of physical infrastructure and difficulty in getting space for the same and poor utilization in middle class and upper middle-class localities. Where established, the OPD attendance is hardly 15-20 patients daily, and may not justify the expenditures on the staff, infrastructure etc. in Bengaluru, Hyderabad &
- In the UPHC the area and population to be covered is indicated, but majority had not mapped their geographical boundaries. None of the UPHC had demarked areas for ASHAs for mobilization activities and some for even Health workers for service provision.
- Almost all states have frozen the qualification for MLHP {B.Sc. (nursing) & BAMS graduates).
- The assessment of additional inputs for identified institutions is yet finalized.
- The capacity development modules particularly for early diagnosis and management of expanded services are yet to be firmed up and integrated with existing training materials of mother and childcare.
- The strategy for capacity building for Nursing graduates in sickness care component at district hospitals has yielded a mixed result.
- For want of either additional human resource or infrastructure, drugs etc. in majority of the health sub-centres HWC’s, running OPD for 6 hours a day has begun. On job supervision and support for centres where CHOs are posted is lacking.
- Under Pradhan Mantri Bharatiya Janaushadhi Pariyojana launched in 2008, Bureau of Pharma Public Sector Undertakings of India (BPPSU), Department of Pharmaceuticals, Govt. of India. Though more than 9400 are currently functional, there is a Paucity of Jan Aushadhalayas averaging to less than 1-2 per Talukas (5650) or Blocks in the country. Where available, access to lifesaving generic drugs at reasonable cost and nearly two thirds of the market prices have improved.
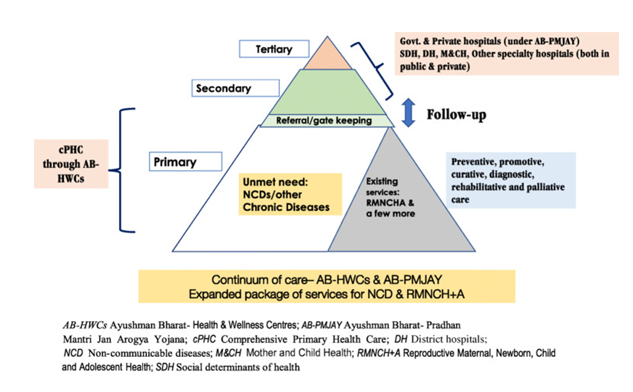
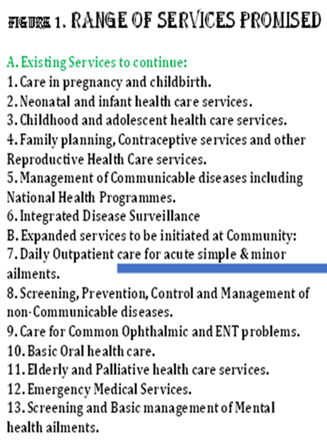
The continuum of the CPHC as promised as represented in the figure below is partially achieved in all most all sates, the difficulty being seen managing sickness cases at HSC and Referral mechanism, optimal home care and community follow-up.
Health is the state of complete physical, mental, and social well-being and not merely the absence of disease, or infirmity and Wellness is an active process through which people become aware of, and make choices toward, a more successful existence. Therefore, NHM assured the services of early identification, basic management, counselling, ensuring treatment adherence, follow up care, ensuing continuity of care by appropriate referrals, optimal home and community follow up, and health promotion and prevention for the expanded range of services.
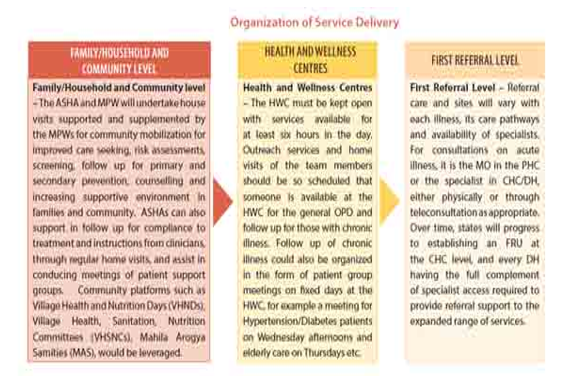
As a first step, Screening, Prevention, Control and Management of Non-communicable Diseases and Chronic Communicable diseases like Tuberculosis and Leprosy has been introduced at HWCs along with Care in pregnancy and childbirth and Childhood and adolescent health care services. The delivery of services for CPHC would be delivered at three levels i.e., i) Family/Household and community levels, ii) Health and Wellness Centres and iii) and Referral Facilities/Sites.
Nurses have a key role to play in primary care in expanding, connecting, and coordinating care. Through their training and work, they are well placed and have been shown to provide safe and effective care in disease prevention, diagnosis, treatment, management, and rehabilitation. This, paper discusses the contribution of CHO only and the challenges phased by them and remedial actions that may have to be taken. Most important of them is of running 6 hours OPD on every working day at SC level Health and Wellness centre against the services promised to continue and expanded services as shown in the table by the side. CHO’s role is discussed in the following heads based on their JD’s:
Care Provider: The nurse muse provides skilled care in clinics and guide Health workers and ASHA’s to provide services at doorstep during home visits.
- Collaborator: CHO is expected to work collaboratively with the health team members in providing health care services.
- Sensitive Observer: The CHO is to be an alert and active observer of surrounding environment changes and natural disasters.
Concerned Adviser: The CHO advises people of the community, on how to handle problematic situations.
Manager: A CHO is to organize and manage various health Program Implementation Plans (PIP) and monitor health activities to achieve planned goals/objectives. - Motivator: CHO must motivate opinion leaders in the community in maintaining health of individuals and environmental health of the villages.
- Leadership: In the absence of a medical officer, the community health Officer is the leader of the health team at the H&WCs.
- Education & Social Mobilization: CHO must promote the health of the community through health education and social mobilization. She empowers for breastfeeding, nutrition, weaning, seeking early care when sick and family welfare services [9].
Where do Nurse-CHO’s stand today?
1. Care Provider: B.Sc. Nursing graduates are posted as CHOs after a bridge course of training in district hospitals. Unfortunately, the skill developed in the course appears to be lacking for primary care as they are taught what is done at the secondary or Tertiary care
hospitals. The Logarithmic approach of classifying the presenting complaints and signs that can be ascertained for conditions like Fevre, cough, headache, constipation, diarrhoea, Insomnia, Itching, Malnutrition, severe conditions needing immediate referral and pre-referral treatments are not being followed. The Male nurses as CHOs are more at loss as their midwifery training is only theoretical and therefore, they are unable to add-value. The skills for assessment of Eye, Ears, Nose, and Throat, mouth, elderly and mental health issues are also found to be inadequate.
Since most of existing health workers are experienced, their skills in the services being continued like ANC, Natal Care, postnatal follow-up, newborn care, nutrition monitoring, often appear to better than new recruits. Emergency medical care and Palliative care and mental health screening and basic management are yet to take off.
2. Collaborator: Collaboration is of 4 types:
i) Communication oriented collaboration dependent on effective communication among team members. The CHOs being new, contractual staff and are less than the regular staff and have average communication skills most of them are finding it difficult. ii) Task-oriented collaboration revolves around achieving specific tasks, goals, or projects and here again the CHOs are finding it difficult to negotiate with health workers.
iii) Network-oriented collaboration: Most health workers are working the current location for 2-20 years and have already established their networks. For the CHOs establishing new networks is difficult unless the local workers are unpopular.
iv) Community-oriented collaboration: creating a sense of community and shared purpose within the workplace. It involves building a positive and supportive team culture, where members collaborate based on shared values and a sense of belonging. CHOs are yet to become an acceptable team member for want of authority, capabilities, and accountability.
3. Sensitive Observer: It is too early to judge n this role as most of them are working in their places for around 2 years, so their observation of environment, outbreaks, and natural disasters for which they are neither trained in B.Sc. (N) nor in induction training. Some of them did contribute in Covid 19 pandemic.
4. Concerned Adviser: Those present during Covid 19 Pandemic 2020-22, played a key and effective role in advising people using masks, washing hands, and avoiding crowd for personal protection against Covid 19 virus. However, this role for handling problematic situation in mother & child nutrition, breast feeding, child development, use of spacing methods of contraception, Dengue and Influenza fevers are yet to be demonstrated.
5. Manager: Most of the working days of CHOs so far have been spent in handling Covid 19 and other vaccinations, and minor ailments treatments. Therefore, preparing PIPs or monitoring progress of activities beyond them like Malaria, Tuberculosis, Hypertension, diabetes, Breast and Cervical Cancer screening, Screening for Myopia, Cataract, mental health - Anxiety and depression etc. for progress towards UHC are yet to be demonstrated.
6. Motivator: Covid 19 Pandemic gave the CHO an opportunity to learn the challenges of motivating opinion leaders in the community in maintaining health of individuals and environmental health of the villages, but consistent involvement of opinion leaders is proving a difficulty after the pandemic. This is one activity where Men CHOs have succeeded better than female CHOs.
7. Leadership: The community health Officers, for want of experience, authority, and better technical and communication skills compared to the other existing senior health workers and worst, their contractual status is finding it difficult to play the role of a leader of the health team at the H&WCs.
8. Education & Social Mobilization: Female CHO’s have contributed to promoting the health of the community through improved quality of ANC, skilled birth attendance wherever labour rooms are there, empowering young mothers for breastfeeding, weaning, nutrition, seeking early care when sick and family welfare services. The men CHO’s are trying to mobilize men for environmental hygiene, elderly care, identifying cataract and screening for diabetes and hypertension but are struggling for want of experience, and involvement local communities, especially of opinion leaders.
Conclusion and Way Forwards
PIPs for CPHC at H&WCs:
The biggest challenge I visualize is the preparation of integrated CPHC plans for HWCs. So far neither Government of India, any states have made any efforts in this direction. This is crucial in a large country where independent vertical programs have pulled and pushed the workers in different directions periodically that confuse them so much that they can take shelter for not doing anything. The development partners like WHO, UNICEF, UNFPA and UNDP may have to take lead in this activity and create model plans for one district in each state and in the process also build state capacities for the same.
Status of running effective Daily OPD’s and Screening for NCDs at HWCs:
The health centres upgraded HWCs will encounter challenges in aspects like infrastructure building, human resource capacity building and drugs other supply logistics. While majority of the Urban H&WCs are underutilised, Rural centres are yet to come up with assurance of extended services. Most importantly making services available at convenient timings of the local population, based on seasonal farming activities, and gaining their trust of the population will demand not only quality services, good behaviour of the service providers and capacities of referral to the appropriate referral institutions and their responses. This calls for a referral mechanism that has been achieved in some vertical interventions like TB, IMNCI, NBC, COPD etc. so far. The HWCs of need Initial support by a medical officer from nearest PHC on weekly basis to provide on job support and brand building.
CHOs need to have skills for i) what to do for a cold, flu, fever, or minor illness in elderly as IMNIC has empowered them for managing these conditions in children, ii) treating tummy upsets- diarrhoea, constipation, Insomnia, Sleep Apnoea among elderly iii) Care of minor injuries decision as to when to refer iv) how to treat a splinter, Nose bleeding, conjunctivitis, mid ear infections, exacerbation of Asthma, Sciatica, Headache, Cough, Fever, Insomnia, Anxiety and Depression.
On job support for these skills are key at the initial stages of CHOs establishing the OPD services, that can be given by medical officers but need to be mandated that each HWW is visited at least once a month.
Screening, Prevention, Control, and Management of NCDS: Screening of Diabetes and Hypertension can be achieved with the support of local medical officer. However, screening for breast, cervical and oral cancers may need specialists visiting at least once a month and therefore may fall short of achievement by 50% by 20230.
Care for Eye and ENT: These services may be just made available by end of 2030 at HWCs only if periodical specialists visits are ensured and CHOs empowered, and a good referral mechanism established and mobilize locals to use these services.
Basic Oral Health Care: Identifying carries and referral is only if a dentist at Block PHC or medical officer (MO) can make weekly visits for on job skill building at the clinics.
Elderly Care: Though the services have begun, HWCs may attend elderly problems of Cataract identification and referral with the optometrist at PHC visiting once a month.
Outbreaks Management: CHO’s need to be analysing the syndromic surveillance data shared by the local health workers and their own OPD data of passive surveillance to identify outbreaks at the earliest, manage the cases and alert community to take up preventive steps like environmental sanitation, use of masks, hand washing etc.
Emergency Services: Some Emergencies during OPD hours are being attended and referred when needed. CHOs have been value add in this intervention, but there is a long way to go! Direct referral mechanism to district or Medical College hospitals will improve the situation.
Screening and Management of Mental Health: NIMHANS run district mental health in Bellary district of Karnataka and some other states gives a hope that at least 50% of primary mental health issues can be tackled at HWCs.
Nursing Colleges and Schools Role to Churn out effective CHO’s:
- Most importantly the Nursing colleges and Schools need to revise their syllabus to equip the graduate nurses to be effective community health Officers.
- This involves adequate clinical skill development exposure both in district and Taluka hospitals and community level PHCs and HWCs.
- It may be good idea to dedicate one entire term in the 4-year degree course and 3 months in internship for exposing to CHOs roles.
References
- Midwives - central to providing quality care to mothers and newborns, during COVID-19 pandemic and beyond, https://www.who. int/India
View at Publisher | View at Google Scholar - T Dileep Kumar, (2010) Growth of nursing in India- Historical and future perspectives,
View at Publisher | View at Google Scholar - Guidelines For Multipurpose Health Worker (Male).
View at Publisher | View at Google Scholar - Pankaj Punjot et.al (2016). Community health officer: the concept of mid-level health care providers, Indian Nursing Council.
View at Publisher | View at Google Scholar - K Suresh (2019) Can India Achieve Universal Health Coverage by 2030? Journal of Quality in Health Care & Economics, Volume 2 Issue 3.
View at Publisher | View at Google Scholar - K Suresh (2022) PUBLIC HEALTH NURSING IN INDIA. Journal of Nur & Res, Volume 3 | Issue 2 | 94
View at Publisher | View at Google Scholar - K. Suresh (2020) Fixing Sickness Care Component of Comprehensive Primary Health Care in India., Journal of Quality in Health care & Economics.
View at Publisher | View at Google Scholar - Key indicators of Social Consumption of India- Health, (2019).
View at Publisher | View at Google Scholar - Health & Wellness, Full Revised Reference Guide.
View at Publisher | View at Google Scholar
