

Research | DOI: https://doi.org/10.31579/2835-835X/093
Efficacy of the therapeutic vaccine VAXIRA® in patients with advanced non-small cell lung cancer: Analysis of integrated clinical trial databases from 2006-2018.
1 Center of Molecular Inmunology. Havana, Cuba
2 Universidad de Las Américas, Quito, Ecuador.
*Corresponding Author: Mayra Ramos-Suzarte, Center of Molecular Inmunology. Havana, Cuba.
Citation: Mayra Ramos-Suzarte, Carmen V. Gonzalez, Marta F. Lopez, Tania C. Ramos, (2024), Efficacy of the therapeutic vaccine VAXIRA® in patients with advanced non-small cell lung cancer: Analysis of integrated clinical trial databases from 2006-2018., Clinical Trials and Case Studies, 3(6); DOI:10.31579/2835-835X/093
Copyright: © 2024, Mayra Ramos-Suzarte. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 October 2024 | Accepted: 31 October 2024 | Published: 07 November 2024
Keywords: non-small cell lung cancer; VAXIRA ®; racotumomab ; overall survival; anti-idiotype vaccine
Abstract
Introduction:
For 20 years, the Molecular Immunology Center has been conducting clinical trials with products aimed at therapeutic targets such as antigens associated with tumor development, especially non-small cell lung cancer (NSCLC). After analyzing more than 3,900 patients in the databases of clinical trials conducted in the country, all the studies were integrated into a single database. It was found that around 20% of patients had a long survival rate, greater than 24 months, when treated with immunotherapies. In a smaller percentage, it was also found that in the group of patients who were controls in these studies, around 10% were also long-term survivors (considering as long-term survivors those who survived more than 24 months after the start of treatment). In the present study, patients included in the following studies were evaluated:Patients included in the Phase II clinical trial of the anti-idiotypic vaccine 1E10 (EC080)
Patients in the non -progressor stratum treated with docetaxel or VAXIRA ® in the Phase III RANIDO clinical trial (EC147). Study period (years): 10 years. September 2006 - December 2016. Purpose of the study: Integrated base of the Phase II and III studies of VAXIRA®. Primary Objective: To identify factors or covariates that may predict long survival in patients with advanced NSCLC after first-line onco -specific therapy treated with the VAXIRA® vaccine.Specific:To compare the overall survival of patients treated with VAXIRA® compared to patients not treated with the vaccine.
Material and Method: This is a database integration study. This study is part of a larger study promoted by the Center for Molecular Immunology (CIM), which integrates the databases of all Cuban patients with advanced stage lung cancer, who have participated in clinical trials with innovative CIM products. This report only includes data from patients who used the VAXIRA® vaccine. The control group was selected for those patients diagnosed with advanced stage non-small cell lung cancer (NSCLC), who participated in one of the included studies, and who, after meeting the same eligibility criteria as patients who received one of the investigational products, were randomly assigned to the group that did not receive it (Phase II of the VAXIRA® EC 080 Vaccine). Patients received VAXIRA® (1 mg), 5 doses intradermally in the induction phase, every 14 days, and in the consolidation or maintenance phase, boosters every 28 days. Patients included in the Phase II clinical trial received treatment for 12 months; patients included in the Phase III trial received treatment with VAXIRA ® as long as the patient's general condition allowed it, regardless of the appearance of disease progression. The study evaluated overall survival as an efficacy variable. Number of patients (analyzed): 321 patients were included in the study. Of these, 180 patients received treatment with VAXIRA®; the rest received no active therapy (89) or received chemotherapy with docetaxel (52). An additional analysis of the patients was performed according to survival time. Long-term survivors were defined as those patients with a survival time greater than or equal to 24 months. Diagnosis and main inclusion criterion: Patients with a diagnosis of advanced non-small cell lung cancer (NSCLC, stage IIIB or IV) confirmed by cytological and/or histological techniques, who at the end of the first line of onco -specific treatment had a response evaluation of stable disease, partial response or complete response (non- progressing patients). All patients included in the present analysis participated in CTs that aimed to evaluate the use of CIM products for the treatment of advanced stage lung cancer.
Results: In the integration of the databases, the median overall survival (global analysis) of patients treated with VAXIRA ® was 9.49 months (95 % CI: 7.57; 11.41). The median survival in the control group was 6.89 months (95 % CI: 5.81-7.98). The difference observed between both groups was statistically significant (p=0.010). The median lifespan of patients treated with Docetaxel was 8.57 months ( 95 % CI: 5.4-11.74). In the group of long-term survivors (54), those treated with VAXIRA® had a higher frequency (70.4%) than patients who received docetaxel (20.4%) or those in the control group who did not receive active treatment (9.3%). It was observed that survival in long-term survivors was higher in the group treated with VAXIRA® than in the rest of the patients (p=0.013). This was demonstrated in the forest analysis plot showing a predominance of survival benefit in patients who received treatment with the VAXIRA ® vaccine. When analyzing by treatment groups, there are certain parameters that benefit the use of the vaccine in relation to chemotherapy and best supportive therapy, such as age, ECOG between 0-1, and adenocarcinoma histological type.
Conclusion:
The median survival (OS) of patients with advanced stage NSCLC who responded to onco -specific maintenance therapy with the vaccine was superior to the overall survival of patients who did not receive treatment. The overall survival (OS) and survival rates of long-term survivors treated with VAXIRA ® were superior to that observed in patients treated with docetaxel and superior to the OS observed in patients who did not receive treatment. Patients who receive the VAXIRA ® vaccine who benefit the most are those with NSCLC histologically classified as adenocarcinomas, stage IIIb disease and ECOG between 0-1
Introduction
Lung cancer is the leading cause of cancer death worldwide. In 2020, a total of 1.7 million deaths were estimated from this cause. The number of new cases estimated in that same year was 2.2 million.1 In Cuba, the situation is equally complex. According to the Cuban Health Yearbook 2021, a total of 5,580 people died from lung cancer in 2020, equivalent to 22.4% of all cancer deaths that year.[2]
With the advent of immunotherapy based on checkpoint inhibitor antibodies and due to the efficacy of these drugs to increase the overall survival of patients with NSCLC treated with them, the United States Oncology community recommends it as Category 1 therapy (highest recommendation) in the NCCN (National Cancer Control and Prevention) standards system. Comprehensive Cancer Netword) by 2024. 3 However, due to the high cost of immune checkpoint inhibitor drugs (ICIs), inhibitors) and their specifications for use, the use of other therapies is maintained, such as chemotherapy, radiotherapy and therapies directed at other specific targets or those associated with tumor development.
It has been reported that the response to first-line platinum-based oncological therapy offers an objective response rate of 25 to 35% and a median survival of 8-10 months in an unselected population, with patients who achieve an objective response or stabilization of their disease having a better prognosis. In this type of patient, it is recommended to use maintenance therapy with the aim of prolonging progression-free survival and overall survival. [3]
There are two types of maintenance therapy: continuous maintenance when at least one drug that was part of the first line of treatment is used, and switched maintenance when one not used in the first line is introduced, always in the absence of disease progression.4 For the selection of maintenance therapy, the treatment received in the first line, the accumulated toxicity due to this cause, the patient's preferences and his general condition must be taken into account.
There are several drugs registered as switch maintenance therapy: among them we can mention docetaxel and pemetrexed. Although recent recommendations are to favor the use of pemetrexed, until 2017 the most commonly used switch maintenance therapy was docetaxel. [3]
Phidias et al reported a Phase III study, where patients who responded to the first line corresponding to 4 cycles of carboplatin- gemcitabine were randomized to receive immediate docetaxel or at the time of progression.5 Overall survival was evaluated as the primary variable, progression-free survival was a secondary variable. A total of 556 patients were included. Patients assigned to the immediate docetaxel arm experienced a significantly longer PFS (5.7 vs 2.7 months, p = 0.001) and a numerically superior overall survival (12.3 vs 9.7 months). Quality of life was assessed using the Lung Cancer Symptom Score (LCSS), the questionnaire was completed by 109 patients in each treatment arm and the results were not statistically different between the groups (p = 0.76).
Other double-blind phase III trials compared immediate treatment with pemetrexed versus placebo after four cycles of platinum-based therapy (not containing pemetrexed), with primary endpoints of PFS and OS as secondary endpoints.6 Eligible patients were randomized 2:1 to receive pemetrexed or placebo and continued the assigned treatment until disease progression, at which time subsequent treatments were assigned at the discretion of the investigator. In the intention-to-treat analysis, pemetrexed significantly improved PFS (4.3 vs 2.6 months) and OS (13.4 vs 10.6 months). Consistent with previous analyses, the benefit of pemetrexed was restricted to patients with non-squamous histology, and in this subgroup it significantly improved both parameters (PFS 4.5 vs 2.6 months, OS 15.5 vs 10.3 months). A significant delay in worsening of symptoms was observed in the arm receiving pemetrexed.
Capuzzo et al conducted a phase III maintenance trial of erlotinib versus placebo in patients who had not experienced disease progression after 4 cycles of first-line platinum-based chemotherapy.[7] The primary endpoints were PFS in all patients and in patients with EGFR-expressing tumors by IHC. OS was assessed as a secondary endpoint. 889 patients were randomized to receive erlotinib or placebo. Patients assigned to receive erlotinib experienced significantly better PFS in the intention-to-treat analysis (12.3 vs 11.1 weeks) and in the EGFR IHC-positive population; and a statistically significant difference in OS (12 vs 11 months).
Due to the demonstrated efficacy of ICI, currently used as first-line treatment, an increase in continued maintenance treatment is observed. In this modality, patients continue with the immunotherapy started at the beginning of treatment.[7]
In the particular case of our country, the high cost of ICI-based immunotherapy prevents our patients from accessing this therapy. In this sense, the possibility of having immunotherapy from our biotechnology industry constitutes a therapeutic alternative and a concrete option for treatments that allow for increased survival in patients with NSCLC.
VAXIRA® vaccine (racotuomab) is an immunotherapy developed by the Center of Molecular Immunology (CIM) for the treatment of patients with Non-Small Cell Lung Cancer (NSCLC) who respond to first-line onco-specific therapy (Switch Maintenance). Alfonso et al. conducted a phase II-III study to evaluate the efficacy of the VAXIRA ® vaccine, as switch maintenance, in 176 patients with advanced NSCLC (EC 080, https://rpcec.sld.cu/trials/RPCEC00000207-En). [8] Patients in the vaccinated group received 1 mg of VAXIRA ® every two weeks for five doses and subsequently re-immunizations every 28 days. In the efficacy analysis by intention to treat, the placebo group had a median survival of 6.80 months vs 8.23 months in the vaccinated group (HR 0.63; 95% confidence interval (CI) 0.46 – 0.87; p = 0.004). The median progression-free survival in vaccinated patients was 5.33 months and 3.90 months for the placebo group (HR 0.73, 95% CI 0.53 - 0.99; p = 0.039). The overall survival rates at one year and two years were 40.2% and 18.4% in the vaccinated group compared with 22.5% and 6.7% in the placebo group (the same formulation of the VAXIRA ® vaccine but without it). 8 In 2013, the health registration certificate was obtained from the Cuban Regulatory Agency. [9]
For 20 years, the Center for Molecular Immunology has been conducting clinical trials with products aimed at therapeutic targets of tumor-associated antigen in non-small cell lung cancer (NSCLC). After analyzing more than 3,900 patients in the databases of clinical trials conducted in the country, it was possible to integrate all the studies into a single database and found that around 20% of the patients had a long survival rate, greater than 24 months, when treated with immunotherapies. In a smaller percentage, it was also found that in the group of patients who were controls in these studies, around 10% were long-term survivors (considering as long-term survivors those who survived more than 24 months after the start of treatment).
The integration of clinical trial databases is a way to obtain more information about a product under investigation, considering the potential of analyzing patients with similar characteristics at different times, but with similar evaluations and potentially compatible objectives. [10] These studies allow the identification of predictive factors of the response to treatments and, in the case of those who are in the control groups, prognostic factors of the disease, which allow a new comprehensive vision to be given to the therapeutic options of a disease.
Materials and Methods
Data integration
Clinical trials generate their own databases, but the number of patients included in each study separately does not always allow us to answer some questions that arise after observing the data. For this reason, procedures have been established to integrate databases of similar studies, with specific criteria for joining them, such as the location of the tumor, the products under study, specific variables, etc. This allows us to provide answers and generate new hypotheses.
Effective data integration allows for improved data quality, systematic data evaluation in each study, and improved data analysis. The Pentaho Data Integration program made it possible to perform data transformation. The components provided by this tool for data transformation allowed all quality problems encountered to be resolved. The development of modular transformation flows in Pentaho Data Integration allowed specialists to work in an organized manner, and each change made to the data was automated, making this process reproducible and auditable. Any specialist can access the transformation flows created by the other specialists and modify or add new changes, such as including new variables in the integration process.[11]
The integration of clinical research on lung cancer from the CIM was carried out. 36 relevant variables were included for this analysis. Using SQL queries (Structured Data Collection System) Query Using the dictionary (Structured Query Language) the models of the clinical trials containing the information were defined and the selected data from each study were loaded. Taking into account the dictionary, the data was cleaned and homogenized for integration. The data of the variables were extracted and stored through a union operation in a new database. The entire process of loading, transforming and integrating data was developed using the Pentaho Data Integration tool , which allowed the traceability of the process to be kept.
Among the variables selected for comparative studies, the following were taken into account: age (over or under 60 years), sex, skin color, smoking habits, histological type, stage of the disease at diagnosis and ECOG.
- Meir curves were estimated for each group of patients according to treatment. The SPSS statistical package version 26 was used.
For each short and long survival subpopulation, the Kaplan Meier curve was adjusted and the log rank test was performed to verify significant differences between groups.
Efficacy variables
Overall survival: Time elapsed from inclusion in the study until death from any cause or date of last news.
Long-term survivor(LS): Long-term survivors were defined as patients who lived 24 months or more.
Short survivor (SS). Survival less than 24 months.
Selection of clinical trials to be included in the integrative analysis
Clinical studies were selected in order to had patients in a control groups and patients treated with the VAXIRA ® vaccine (racotumomab). Those clinical trials (CT) were carried out between the period of 2006 and 2018, in patients with NSCLC, with similar characteristics, who had received the first line of oncological therapy, in stage IIIb or IV of the disease and who had been non- progressors. In that sence were selected two CT:
- Multicenter clinical trial, randomized, stratified, open and compared in patients with advanced NSCLC treated with Racotumomab or Nimotuzumab, vs Docetaxel after first line treatment oncospecific. Phase II clinical trial of the anti-idiotypic VAXIRA ®, (EC-080), https://rpcec.sld.cu/trials/RPCEC00000207-En , Unique ID number: RPCEC00000207.
Study centers:
Phase II clinical trial (EC-080):
- Hermanos Ameijeiras Hospital. Havana.
- Faustino Perez Hospital, Matanzas
- Celestino Hernandez Hospital, Villa Clar
- Multicenter clinical trial, randomized, stratified, open and compared in patients with advanced NSCLC treated with Racotumomab or Nimotuzumab, vs Docetaxel after first line treatment oncospecific. Phase III RANIDO (EC-147). https://rpcec.sld.cu/trials/RPCEC00000179-En; Unique ID number: RPCEC00000207
Included patients in 24 hospitals and 57 polyclinics in 14 cuban provinces.
Study Centers:
- Hermanos Ameijeiras Hospital (Havana)
- National Institute of Oncology (Havana)
- Julio Trigo Hospital (Havana)
- Enrique Cabrera Hospital (Havana)
- Miguel Enriquez Hospital (Havana)
- Joaquin Albarran Hospital (Havana)
- Manuel Fajardo Hospital (Havana)
- Jose R. Lopez Tabranes Hospital (Matanzas)
- Celestino Hernandez Robau Hospital (Villa Clara)
- Gustavo Aldereguía Lima Hospital (Cienfuegos)
- III Congress Hospital (Pinar del Rio)
- Commander Pinares Hospital (Artemisa)
- Camilo Cienfuegos Hospital (Sancti Spiritus)
- Antonio Luaces Iraola Hospital (Ciego de Avila)
- Roberto Rodriguez Hospital (Ciego de Avila)
- Maria Curie Hospital (Camagüey)
- Manuel Ascunce Domenech Hospital (Camagüey)
- Ernesto Guevara Hospital (Las Tunas)
- Vladimir I. Lenin Hospital (Holguin)
- Agostino Neto Hospital (Guantanamo)
- Carlos M. Cespedes Hospital (Granma)
- Celia Sanchez Manduley Hospital (Granma)
- Saturnino Lora Hospital (Santiago de Cuba)
- Juan Bruno Zayas Hospital (Santiago de Cuba)
Study period (years):
September 2006 - December 2018
Purpose of the study: Integrated base of the Phase II and III studies of VAXIRA® vaccine
Principal Endpoint:
To identify factors or covariates that may predict long survival in patients with advanced NSCLC after first-line onco -specific therapy treated with the VAXIRA® vaccine.
Specific objetives:
To compare the overall survival of patients treated with VAXIRA® compared to patients not treated with the vaccine.
To compare overall survival in patients with short and long overall survival after treatment with VAXIRA® with untreated patients.
Diagnosis and main inclusion criterion: Patients with a diagnosis of advanced non-small cell lung cancer (NSCLC, stage IIIB or IV) confirmed by cytological and/or histological techniques, who at the end of the first line of onco -specific treatment had a response evaluation of stable disease, partial response or complete response (non- progressing patients). All patients included in the present analysis participated in CTs that aimed to evaluate the use of CIM products for the treatment of advanced stage lung cancer.
Investigational product, dose and schedule of treatment: Patients in the VAXIRA ® vaccine arm (racotumomab), in the present database integration (n=180) were included in the Phase II clinical trial (CT) EC080 (n=87) and the Phase III CT EC-147 (n=93). The therapy received consisted of five doses intradermally every 14 days and subsequently, reimmunizations every 28 days until reaching almost 15 doses. These patients could continue treatment with the vaccine as long as their general condition permitted it, even beyond the progression of the disease.
One group of patients received docetaxel (as standard chemotherapy in Cuba for maintenance therapy) from CT EC-147 (which for the purposes of this study will be the docetaxel group) and another group was assigned to receive the best available treatment, for the purposes of this analysis this group is called the control group, from the clinical trial EC-080.
Evaluation criteria: All patients who were included in the referred studies were selected, always by Intention to Treat (ITT), and who also met the following inclusion criteria: confirmed cytological or histological diagnosis of advanced NSCLC carcinoma, stage IIIB or IV, who have signed the informed consent, who have achieved a favorable response (complete, partial response or stable disease) at the end of the first standard line of CT/RT. Patients whose time interval between the end of the onco -specific treatment and the start of vaccination is between 28 and 56 days, age between 18 and 75 years, both inclusive, general condition according to ECOG £2 ( Karnofsky ³60%) with normal organ function and life expectancy of four months or more.
Overall survival: Estimated in months from the date of inclusion in the studies until death from any cause or the date of last news in the integrated database.
Results
Sample Description
Table 1 presents the composition of the sample selected for the analysis of the integrated databases. EC-080 was the Phase II EC where the VAXIRA ® vaccine was compared with placebo and the results of this study gave the Vaxira® vaccine conditional registration for the first time in 2013.[8] The placebo had the rest of the components of the vaccine formulation, except for the VAXIRA ® AcM (specific salts of the formulation and alumina).[9] The EC-147 (RANIDO), was a non-inferiority clinical trial, Phase III, in which it was proposed that the administration of the VAXIRA® vaccine and the humanized AcM nimotuzumab were non-inferior to the switch maintenance therapy established in Cuba and in the NCCN in the year in which it was designed ( docetaxel ), so no differences were expected between the treatments, although there were in safety, with a benefit expected in terms of adverse reactions related to the research products in relation to the switch maintenance chemotherapy.[4]
For patient selection:
A retrospective cohort study was designed, a cohort of patients treated with VAXIRA ® , another with Docetaxel and another of untreated patients (Controls), concurrent in time.
To evaluate the homogeneity between the cohorts in terms of demographic variables and disease characteristics, the Chi-square test was applied using SPSS Version 25 software. This study presents the results of a data set according to the distribution of demographic variables (age, sex, skin color and smoking habits) and disease characteristics (histological type, stage and ECOG).
Number of patients (analyzed): 321 patients were included in the study. Of these, 180 patients received treatment with VAXIRA®, the rest received no active therapy (89) or received chemotherapy with docetaxel (52). An additional analysis of the patients according to survival time was performed. Long-term survivors were defined as those patients with a survival time greater than or equal to 24 months. The final result of this analysis in scenario three, yielded a sample of 321 patients (table 1).
Clinical trial
| Treatment groups | Total | ||
| Control | Docetaxel | VAXIRA® | ||
| EC080 | 89 | 0 | 87 | 176 |
| EC147 | 0 | 52 | 93 | 145 |
| Total | 89 | 52 | 180 | 321 |
Table 1. Frequency distribution of patients according to trial and treatment group.
The general demographic characteristics of the selected patients are shown in Table 2. It is important to note that the sample is balanced, no difference is observed for the three groups in any of the variables that could predict the response to the treatments, except for the Stage of the disease, and when analyzing the proportions, the difference is observed fundamentally in the chemotherapy group since the control group and the group treated with the vaccine have similar proportions.
Overall Survival.
Figure 1 shows the Kaplan Meier curve for overall survival in patients included in the study in each of the groups globally. A superiority was obtained in the median and overall survival rates of the VAXIRA ® group with respect to the other two. It can be seen that, in the survival rates up to 48 months, the VAXIRA ® group benefits, although this superiority becomes minimal in the rates at 24 months, where it is superior to the control, but the difference with Docetaxel only shows non-inferiority. This difference is accentuated over time, showing an advantage for the Vaxira vaccine.
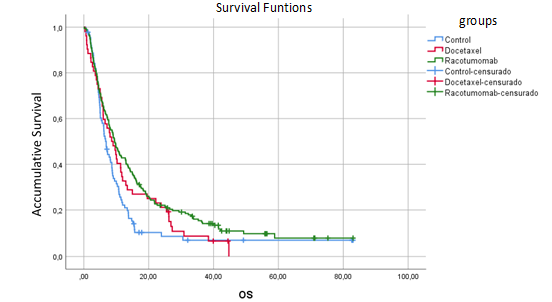
Figure 1. Kaplan Meier curve of overall survival in patients included in the study.
| Group | N | Number of events | Censored | Median months | Std . Error | 95% confidence interval | Log- rank | |||||||
| N | % | Lower limit | Upper limit | p-value | ||||||||||
| Control | 89 | 80 | 9 | 10.1% | 6,899 | ,551 | 5,819 | 7,980 | 0.010 | |||||
| Docetaxel | 52 | 49 | 3 | 5.8% | 8,575 | 1,619 | 5,402 | 11,748 | ||||||
| VAXIRA® | 180 | 159 | 21 | 11.7% | 9,495 | ,980 | 7,575 | 11,415 | ||||||
Groups
| Survival Rate | |||||||||||||
| 12 months | 24 months | 36 months | 48 months | |||||||||||
| Control | 22.1 | 8.5 | 6.8 | 6.8 | ||||||||||
| Docetaxel | 32.7 | 21.2 | 8.5 | 6.4 | ||||||||||
| VAXIRA® | 42.8 | 22.1 | 15.3 | 10.8 | ||||||||||
Long-term survival analysis
Table 3 shows the distribution of patients according to survival time. Most patients had an overall survival of less than 2 years (83.2%), while long-term survivors accounted for 16.8% of the total integrated sample. With respect to the total number of long-term survivors, the largest number of long-term survivors (70.4%) were in the VAXIRA ® vaccine group, but proportionally with respect to the treatments under evaluation, both chemotherapy and vaccine had similar proportions. Considering that EC 147 was a non-inferiority trial with Docetaxel, the robustness of this result is confirmed (Table 3).
Table 3. Clinical characteristics of the included patient Distribution of the patient population treated in the course of the clinical trials evaluated according to the assigned treatment group and duration of survival.
| Treatment Group | Control N=89 | Docetaxel N=52 | VAXIRA® N= 180 | Total* N=321 |
| Short Survivors | 84 (94.4 %) | 41 (78.8 %) | 142 (78.9 %) | 267 (83.2%) |
| Long Survivors | 5 (5.6 %) | 11 (21.2%) | 38 (21.1%) | 54 (16.8%) |
*Proportions are calculated in relation to the total number of patients per column.
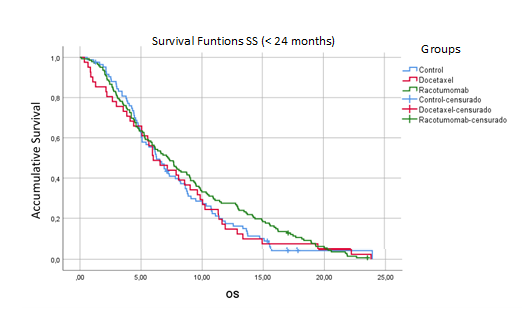
There were no significant differences between the groups in the short survival subpopulations (Figure 2; p=0.435). The 18-month survival rates were in “numerical” benefit of the VAXIRA ® vaccine group (Figure 2).
Group
| Total N | Number of events | Censored | Median months | Std. Error | 95% confidence interval | Log-rank test | ||
| N | % | Lower limit | Upper limit | p-value | |||||
| Control | 84 | 79 | 5 | 6.0% | 6,275 | ,632 | 5,037 | 7,513 | 0.435 |
| Docetaxel | 41 | 41 | 0 | 0.0% | 6,012 | ,967 | 4,116 | 7,908 | |
| VAXIRA® | 142 | 140 | 2 | 1.4% | 7,195 | ,697 | 5,828 | 8,562 | |
Group
| Total N | Number of events | Censored | Median months | Std. Error | 95% confidence interval | Log-rank test | ||
| N | % | Lower limit | Upper limit | p-value | |||||
| Control | 84 | 79 | 5 | 6.0% | 6,275 | ,632 | 5,037 | 7,513 | 0.435 |
| Docetaxel | 41 | 41 | 0 | 0.0% | 6,012 | ,967 | 4,116 | 7,908 | |
| VAXIRA® | 142 | 140 | 2 | 1.4% | 7,195 | ,697 | 5,828 | 8,562 | |
| Survival Rate | 6 months | 12 months | 18 months |
| Control | 55.4 | 17.4 | 4.3 |
| Docetaxel | 51.2 | 14.6 | 7.3 |
| VAXIRA® | 56.3 | 27.5 | 10.4 |
Figure 2. Kaplan Meier curves of overall survival according to short survivors (less than 24 months of survival) in patients included in the study.
When analyzing the long-term survivor group, significant differences were observed between the groups analyzed (Figure 2a), p=0.014. The placebo control group was not taken into account since it only had 5 long-term survivors. It is notable that the survival rates of patients treated with the VAXIRA® vaccine exceeded the rest of the groups, the probability of being alive at 60 months was 34.9%, while those treated with chemotherapy did not survive beyond 36 months (Figure 2a).
Groups
| Total N | Number of events | Censored | Median months | Std . Error | 95% confidence interval | -rank test | ||
| N | % | Lower limit | Upper limit | p-value | |||||
| Docetaxel | 11 | 8 | 3 | 27.3 | 30.9 | 3.1 | 24,839 | 36,927 | 0.014 |
| VAXIRA® | 38 | 19 | 19 | 50.0 | 42.2 | 5.4 | 31,697 | 52,738 | |
Groups | Survival Rates % months | |||
| 24 | 36 |
48 |
60 | |
| Docetaxel | 90.9 | 30.3 | 0.0 | 0.0 |
| VAXIRA® | 97.4 | 66.6 | 49.1 | 34.9 |
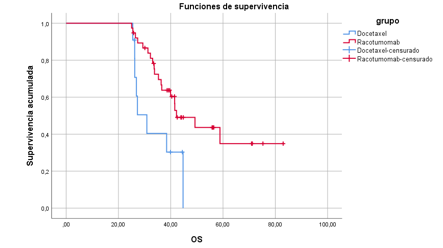
Figure 2a. Kaplan to Meier curves of overall survival for patients with survival greater than 24 months (long-term survivors) included in the integrated database study.
Subgroup analysis (forest plot)
Subgroup analysis (forest plot). Overall population of patients treated with VAXIRA ® vs control.
All patients from the selected clinical trials databases were evaluated, integrated globally, analyzing those vaccinated with VAXIRA ® vs. controls.
A benefit to the vaccine is observed for all parameters analyzed, except for ECOG 2, mixed skin and ex-smokers. Patients with this ECOG have a more unfavorable clinical status than those with a lower performance status. This patient has a more unfavorable status to receive any type of therapy, so their immune system could also be in a more compromised situation to respond to a vaccine and not raise antibodies against it, this being the mechanism of action of therapeutic vaccines (Figure 3).
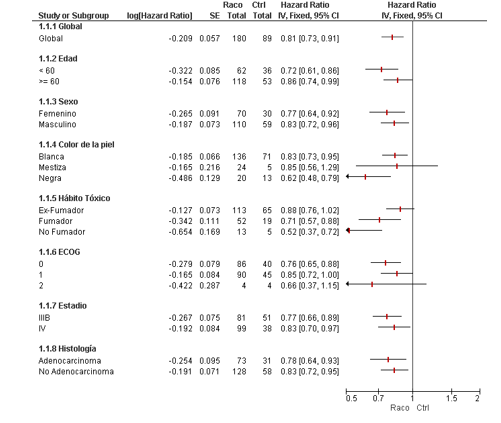
Figure 3. Subgroup analysis. Overall population. Vaxira vs Control
Patients with lower ECOG have not only a more immunocompetent immune system, but better conditions to receive therapies from a clinical point of view in general.
Subgroup analysis (forest plot). Overall population of patients treated with VAXIRA ® vs docetaxel.
Patients who received docetaxel maintenance chemotherapy were compared with those who received the VAXIRA ® vaccine. The study in which docetaxel was used was non-inferiority. The objective of this study (RANIDO Phase III, EC 147), was to demonstrate the non-inferiority of
the vaccine in relation to the established chemotherapy as switch maintenance therapy (docetaxel), with which a large number of adverse reactions were reported, allowing only the administration of a certain number of cycles. With this, the substitution of this chemotherapy by the VAXIRA ® vaccine was proposed, given the safety reported in previous studies [8-9,11-13] and to avoid the adverse reactions associated with docetaxel. [5-6]
This comparison showed that non-smokers, stage IIIb disease and histologically classified as adenocarcinomas, had a benefit from the use of the VAXIRA ® vaccine. (Figure 4)
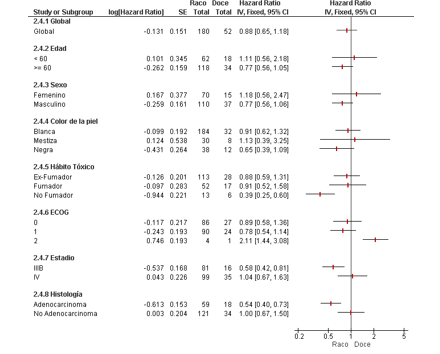
Figure 4. Subgroup analysis. Overall population. VAXIRA ® vs. Docetaxel.
Subgroup analysis. Short-term survivor population. (VAXIRA ® vs docetaxel).
For patients with survival less than 24 months (short survivors), a marked benefit was observed in favor of those patients who received the VAXIRA ® vaccine if they were under 60 years of age, had black skin, and were ex-smokers (Figure 5).
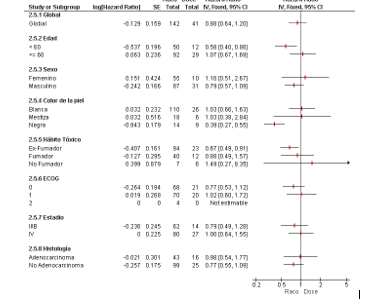
Figure 5. Subgroup analysis. Short-term survivor population. Vaxira vs Docetaxel.
Subgroup analysis. Long-term survivor population. (VAXIRA ® vs docetaxel)
The analysis was carried out for long-term survivors (survival greater than/equal to 24 months) in which, in general, a benefit was observed for all patients treated with the vaccine, highlighting those over 60 years of age, white skin, smokers, stage IIIB and adenocarcinomas (Figure 6).
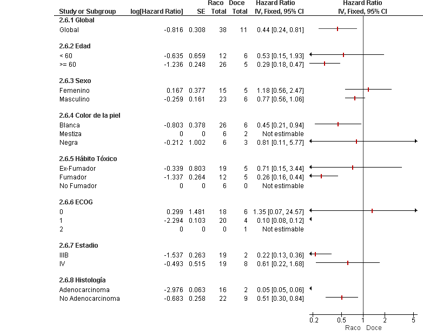
Figure 6. Subgroup analysis. Long-term survivor population. Vaxira vs Docetaxel.
Discussion
The population included in this study was balanced, showing no differences between the groups and parameters analyzed, except for the stage of the disease at diagnosis (being at a disadvantage for the groups that received chemotherapy). In the case of the control and VAXIRA ® groups, patients with stage IIIB of the disease predominated, while in the Docetaxel group, patients with stage IV of the disease predominated (statistical differences were observed), which reflects a greater degree of disease progression and a worse prognosis for this group.
In this study we observed that patients treated with VAXIRA ® had a survival of 9.49 months (95% CI: 7.5-11.4), statistically superior to that reported in the two remaining groups (p= 0.010). These results in the overall SV are similar to those obtained by Alfonso et al. in a controlled clinical trial comparing the efficacy of the vaccine vs placebo in patients with advanced stage NSCLC (IIIB-IV) as a switch maintenance.8 In this study, treatment with VAXIRA ® demonstrated its superiority (HR: 0.63, 95% CI 0.63-0.87) with a median overall survival of 8.23 months vs 6.80 in the placebo-treated control group.
Similarly, the overall survival median reported in this study of the use of VAXIRA ® in the real world is similar to that reported more recently by Hernandez et al [11]. These authors report the results of a randomized, controlled Phase III clinical trial comparing VAXIRA ® and nimotuzumab with docetaxel as a switch maintenance treatment in NSCLC. In this study, the median overall survival was 9.8 months (95%CI=8.8-13.7)
Until the introduction and acceptance of maintenance therapies, the treatment of patients with advanced NSCLC did not include the use of other drugs after the initial systemic treatment. Hence, the first studies with VAXIRA ® (and CIMAvax -EGF®) in this setting included the use of placebo or best supportive care as a control group.
Currently, NCCN experts in 2024 continue to recommend the use of platinum combinations as drugs “useful in certain conditions” in patients with metastatic lung cancer, especially in cases of contraindications to immunotherapy. The specific recommendation is that chemotherapy be used in patients with negative diagnostic tests for the presence of “driver” mutations.[3]
Among the three treatment groups studied, the VAXIRA ® group had the highest frequency of long-term survivors (70.4%).
The high survival rates observed in our study, particularly from 24 months and beyond, support the study previously reported by Sánchez et al. In this study, long-term lung cancer survivors after treatment with VAXIRA ® showed an increase in their overall survival duration (more than six years) much higher than that observed in the group of long-term survivors not treated with VAXIRA ® (close to three years).[9]
The results presented in this integrated database study confirm the data obtained in each of the separate studies, where the survival of the VAXIRA ® vaccine is superior to the groups analyzed and greater than 9 months. This demonstrates the consistency of the processing and analysis of the same, in two different scenarios. A greater benefit in terms of survival is reported in all subgroups of patients treated with VAXIRA ® when compared to the control group.
When comparing patients who received the vaccine vs. those who received maintenance chemotherapy (docetaxel), it was observed that non-smoking patients, patients with adenocarcinomas and stage IIIb disease benefited from it (Figure 4). In this same group of patients analyzed, but in the case of patients who have a survival of less than 24 months (short survivors), there is a benefit in favor of those patients who received the VAXIRA® vaccine if they were under 60 years old, ex-smokers and black (Figure 5), while for long survivors a benefit was observed in favor of the VAXIRA® vaccine in all patients who received it and also those who were over 60 years old, white skin and smokers. (Figure 6).
The fact that there is a group of patients in the study who are long-term survivors (16.8%) is consolidated, and of these, 70.4% are those treated with the VAXIRA ® vaccine. The probability that a patient treated with the Vaxira vaccine is alive 60 months after starting treatment (from the subgroup of long-term survivors) is 34.9%, while those who received chemotherapy or docetaxel do not survive beyond 36 months.
Conclusion
An integrated analysis of the databases of two clinical trials (Phase II and Phase III) was performed, weighting the patient groups and analyzing the different therapies received. The median survival of patients with advanced stage NSCLC who respond to onco -specific maintenance therapy, treated with VAXIRA ®, is higher than the overall survival of patients who do not receive active treatment and the best supportive therapy. The overall survival and survival rates of long-term survivors treated with VAXIRA ® are higher than those observed in patients treated with docetaxel and higher than the overall survival observed in patients who do not receive active treatment. In general, those patients who receive the VAXIRA ® vaccine who benefit the most are those with adenocarcinomas of the NSCLC, in stage IIIb of the disease and ECOG between 0-1.
Author Contributions: Conceptualization: M.R., C.V., M.F., T.C.; Data curation: M.R., C.V.; Formal analysis: M.R., C.V., M.F., T.C.; Researchs: M.R., M.F., T.C.; Methodology: M.R., C.V.; Project administration: M.R., T.C.; Material resources: M.R., M.F.; Supervision: M.R.,T.C.; Validation: M.R., C.V., M.F.; Visualization: M.R., T.C.; Writing – original draft: M.R.,T.C.; Writing – review and editing: M.R., C.V., M.F, T.C.
Conflict Of Interest: The authors declare no conflicts of interest.
References
- Ohe, Y., Kubota, K., et al. (2007). Randomized phase III study of cisplatin plus irinotecan versus carboplatin plus paclitaxel, cisplatin plus gemcitabine, and cisplatin plus vinorelbine for advanced non-small-cell lung cancer: Four-Arm Cooperative Study in Japan. Annals of Oncology, 18, 317-323.
View at Publisher | View at Google Scholar - WHO, Global Observatory of Cancer. 2020.
View at Publisher | View at Google Scholar - MINSAP, Anuario Estadístico de Salud. 2021.
View at Publisher | View at Google Scholar - NCCN, NCCN Guideline Version 3 Non-Small Cell Lung Cancer. 2024.
View at Publisher | View at Google Scholar - Fidias, P., DeVore, S., Lyss, A.P., et al. (2009). Phase III study of immediate compared with delayed docetaxel after front line therapy with gemcitabine plus carboplatin in advanced non-small cell lung cancer. Journal of Clinical Oncology, 27, 591-598.
View at Publisher | View at Google Scholar - Ciuleanu, T., Brodowicz, T., Belani, C.P., et al. (2008). Maintenance pemetrexed plus best supportive care versus placebo plus best supportive care: A phase III study. Proceedings of the American Society of Clinical Oncology, 8011.
View at Publisher | View at Google Scholar - Cappuzzo, F., Ciuleanu, T., Stelmakh, L., et al. (2010). Erlotinib as maintenance treatment in advanced non-small cell lung cancer: a multicentre, randomised, placebo-controlled phase 3 study. Lancet Oncology, 11, 521-529.
View at Publisher | View at Google Scholar - Cecmed, Certificado de registro sanitario. 2013.
View at Publisher | View at Google Scholar - Alfonso, S., et al. (2014). A randomized, multicenter, placebo-controlled clinical trial of VAXIRA® -alum vaccine as switch maintenance therapy in advanced non-small cell lung cancer patients. Clinical Cancer Research, 20(14), 3660-3671.
View at Publisher | View at Google Scholar - van der Steen, J.T., et al. (2008). Benefits and pitfalls of pooling datasets from comparable observational studies: combining US and Dutch nursing home studies. Palliative Medicine, 22(6), 750-759.
View at Publisher | View at Google Scholar - Hernandez, M., Ortiz, RA, Salomón, E., et al. (2022). Safety and efficacy of CIMAvax-EGF vaccine for the treatment of real-world non-small cell lung cancer patients. International Clinical Medicine.
View at Publisher | View at Google Scholar - Viada, C., Bouza, C., Ballesteros, J., et al. (2018). Quality of life assessment as a predictor of survival in cancer. Bionatura , 5(3).
View at Publisher | View at Google Scholar - Viada, C., Vega, A.M., Robaina, M., et al. (2020). Evaluation of Nimotuzumab for the treatment of head and neck cancer: Meta-analysis of controlled trials. Bionatura , 5(1).
View at Publisher | View at Google Scholar - Hernandez, M., Neninger, E., Ortiz, RA, et al. (2021). Safety and Efficacy of Racotumomab-alum or Nimotuzumab versus Docetaxel as switch maintenance therapy for advanced non- small cell lung cancer patients: a Phase III open label randomized non-inferiority trial. Global Surgery , 7.
View at Publisher | View at Google Scholar
