

Research Article | DOI: https://doi.org/DOI:10.31579/2835-835X/032
Comparative Case Report of the Application of Poly-L-Lactic Acid in two Different Presentations for the Treatment of Flaccidity in the Medial Region of the Arms
*Corresponding Author: Josiane Duarte da Silva, Viana, Espirito Santo · Current city · Vitória, Brazil · Hometown.
Citation: Josiane Duarte da Silva, (2023), Comparative Case Report of the Application of Poly-L-Lactic Acid in two Different Presentations for the Treatment of Flaccidity in the Medial Region of the Arms, Clinical Trials and Case Studies, 2(4); DOI:10.31579/2835-835X/032
Copyright: © 2023, Josiane Duarte da Silva. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 July 2023 | Accepted: 20 July 2023 | Published: 07 August 2023
Keywords: aging; skin; collagen; body contouring; esthetics
Abstract
To conduct a clinical assessment, in the same patients, the action of poly-L-lactic acid of two different presentations in the treatment of body skin flaccidity of the inner region of the arms.
Patients and methods: Samples were collected from 4 patients aged between 18 and 65 years. The patients underwent application of poly-L-lactic acid in two different presentations: Rennova Elleva® (Ghana R&D CO, LTD – South Korea) and the comparator product, Sculptra®, Galderma S.A. (Switzerland). After the applications, the results were monitored via photography and ultrasound evaluation 3 and 6 months after the application. The results were submitted to statistical analysis using GraphPad Prism 9.0® software (USA). Results with p<0.05 were considered significant.
Results: The comparison between the products showed that in terms of sagging, the visual evaluation showed that the comparator product did not show a relative improvement in sagging. In contrast, Rennova Elleva® was possible to observe visual improvement in sagging in the arms. Statistically, no results associated with sagging were observed (p>0.05).
The evaluation of the products in the improvement of the epidermal-dermal thickness, showed that Rennova Elleva® improved significantly, while the comparator product did not present improvement in this evaluation pattern. There was a statistical statistic in the comparison between groups, demonstrating that Rennova Elleva® was better than the comparator product(p<0.05).
Conclusion: The application of poly-L-lactic acid to improve sagging facial and body skin is already well known. The results showed that there was a statistically significant increase in the epidermal- dermal thickness where Rennova Elleva® was applied. It is suggested that for future studies, a larger number of patients be used.
Introduction
The changes observed in the chronological aging of the skin are the result of a normal physiological process and are caused by epidermal, dermal and hypodermal thinning, which, in turn, are aggravated by photoaging.[1]. In the body, in addition to aging, a number of other factors contribute to the appearance or worsening of skin flaccidity, such as restrictive diets that are low in protein, rapid weight loss and low BMI, liposuction, post-pregnancy, and the presence of stretch marks, which favor the loss of skin elasticity, even among young patients. [2,3].
New and innovative treatments for skin aging are constantly evolving, with various studies published on the treatment of body flaccidity. [2,3,7].
In chronological aging, changes occur in the mechanical properties of the skin, which include the progressive loss of elasticity, with a prolongation of the time needed to return to the original state after pinching, caused by biochemical and structural changes in collagen, elastic and ground substance fibers. [1,4].
In addition to aging, the body undergoes the stretching of the skin caused by pregnancy and weight gain; the presence of stretch marks that arise from the rupture of collagen fibers and disorganization of elastic fibers[11]. and thinning of the hypodermis due to loss of adipose tissue caused by weight loss and high-performance sports practice, with a decrease in BMI [12]., which also determine the appearance of flaccidity even among younger patients. On clinical examination, the skin appears wrinkled, loose, and with depressions on the surface. On palpation, the skin becomes thin and inconsistent.
Women are more affected by flaccidity for several reasons: the dermis in women is thinner;1 in men, the fibrous septa in the hypodermis are smaller and arranged in oblique planes, with small lobes of fat, while in women, the lobules are larger and with parallel septa, offering less resistance to stretching;[12]. in women, the reduction in serum estrogen levels observed after the climacteric period leads to even more skin extensibility and less elasticity, and as a consequence, clinically, the skin appears thinner, drier, and more flaccid;[13]. women undergo more situations during life that result in skin stretching, such as pregnancy. Flaccidity may also be aggravated by patients’ lifestyle habits, such as smoking, restrictive diets, and rapid weight changes.
Once sagging is installed by changes in collagen and elastic fibers of the dermis and hypodermis, the ideal treatment should be based on neocollagenesis to ensure better results. This is the mechanism of action of poly-L-lactic acid (PLLA): to induce a local and gradual reaction that leads to the recovery of the collagen network modified during the aging or stretching process.
PLLA is an injectable synthetic polymer from the alpha-hydroxy acid family, being biocompatible and biodegradable, with very low cytotoxicity.[5]. Kulkarni et al. (1966) demonstrated that the degradation of poly-L-lactic acid (PLLA) could occur in vivo, and since then, it has been used in the medical field, mainly in the production of sutures, stents, and as a vehicle in microspheres for drug delivery. This material, in injectable form, has been applied as a cosmetic filler since 1999, with many studies being published attesting to its safety, effectiveness, and longevity. [4,5].
The injections of its microparticles in the deep dermis or superficial hypodermis induce a local and gradual reaction by the fibroblasts with the formation of new collagen and subsequent increase in dermal thickness. This fibroplasia determines the recovery of the lost collagen support network structure and the improvement of skin flaccidity with excellent cosmetic results. [4-6]. As the results of PLLA treatment occur gradually, depending on tissue response and biological processes, they may not be evident for weeks after application. Therefore, it is crucial to wait for the biological response to occur between each application, with additional treatment sessions being done at intervals of at least 4 weeks between them. [2-6]. The response time and degree of improvement of the correction depend essentially on the individual response of each patient, which in turn may vary according to age, sex, skin quality, phototype, and eating habits.[4].
The purpose of this study is to assess and compare the clinical response of two PLLA presentations available and approved by regulatory bodies for the treatment of skin flaccidity. The treatment was performed on the inner part of the arms in the same patients.
Material and methods:
Study participants:
The study protocol was reviewed and approved by Research Research Ethics Committee. The study was conducted in accordance with the Ethical Standards of the National Committee for Ethics in Research with Human Beings, which follows the principles of the Declaration of Helsinki. The approval number is: 5.761.855 (CAAE:60626622.4.0000.0082). All patients were in agreement with the Informed Consent Form, as well as with the scientific publication of the data obtained through data collection.
The inclusion criteria were: Women aged 18 to 65 years with flaccidity in the indicated area, with a stable weight in the last six months. In the case of women of childbearing age: use of some contraceptive method.
The exclusion criteria were: Women under 20 or over 65 years old, who presented any of the following conditions: pregnancy and lactation, vegetarian or vegan diet, weight loss, hypertension, metabolic diseases and diabetes, inflammatory and autoimmune diseases, use of steroids or other routine anti-inflammatory drugs in the last 6 months, skin diseases, and allergies.
Classification of the degree of flaccidity:
The score for the degree of flaccidity used was based on the SLSS (Skin Laxity Score System) scale by Blyumin-Karasik et al. (Table 1).[8]. Based on the scale, patients with intermediary scale were rounded down
| Degree | Description |
| 0 | Toned skin.Firm with smoothskin surface texture. |
| 1 | Skin slightly smooth. Slightly tonedwith smooth skin surface texture. |
| 2 | Moderately looseskin. Slightly wrinkled with crackles on the skinsurface. |
| 3 | Very looseskin without tone,highly wrinkled withcrackles, separating the skin fromthe subcutaneous tissue. |
| 4 | Prominent redundance of the skin, without tone, highly wrinkled, with crackles on the surface of the skin. |
Table 1: SLSS Scale – Scoring system for assessing skin flaccidity.
Products:
Currently, two commercial presentations of poly-L-lactic acid are approved by regulatory agencies for the treatment of skin flaccidity: the comparator product (Sculptra®, Galderma
S.A. – Switzerland), which comes in the form of a white lyophilized powder compacted at the bottom of a clear, colorless bottle, containing 150 mg of PLLA particles, 90 mg of croscarmellose (CMC) to disperse the particles, and 127.5 mg of pyrogenic mannitol, prepared 24-48 hours before application;5 and Rennova Elleva® (Ghana R&D CO, LTD – South Korea), which is presented in the form of a lyophilized dispersed powder in a clear amber colored vial, containing 210 mg of poly-L-lactic acid (PLLA) microparticles (+40%), 132 mg of carboxymethylcellulose (CMC) (+47%), and 178 mg of pyrogenic mannitol (+40%), with preparation recommendeone hour before application. [7]
Product preparation:
Both vials were reconstituted 24 hours prior to application with distilled water for injection using
10 ml for the comparator product and 14 ml for Rennova Elleva®. The vials were stored under refrigeration. At the time of application, the products were diluted with distilled water, totaling 16 ml for the
comparator product and 22.4 ml for Rennova Elleva®, corresponding to a concentration of 9.37 mg of PLLA per milliliter for both presentations.
Patient preparation:
The selected patients signed a Free and Informed Consent Form and answered a questionnaire about the degree of flaccidity they presented, according to the SLSS (Skin Laxity Score System) scale by Blyumin-Karasik et al.
Photographic documentation was performed in four positions for both arms: front and back at rest and in muscle contraction, in addition to skin plication to assess skin distension. High-resolution ultrasound examination with a high-frequency transducer (18 MHz) was performed using the Logiq® device (GE Healthcare, Pittsburgh, PA) in eight quadrants for each arm. [9-10]. In each quadrant, 5 measurements of the thickness of the epidermis-dermis were conducted in a continuous way, with a spacing of about 0.1-0.2 cm between measurements. The inner part of the forearms was demarcated into 8 quadrants measuring 5 cm x 5 cm, according to the scheme presented in Figures 1A and 1B.
Anesthetic cream with 7% lidocaine and 7% tetracaine was applied thirty minutes prior to the applications. The mean value of each quadrant was calculated at pre-treatment, 3 months after treatment, and 6 months after treatment.
Applications:
After rigorous cleaning with chlorhexidine, 2 ml were applied in each quadrant in a fan with 0.4ml by retrograde injection, totaling 16 ml of each product (150 mg of PLLA) in each arm. the comparator product was applied on the right arm, while Rennova Elleva® was applied on the left arm of all patients. The applications were made by the same applicator and with the same technique, using 22G x 7 cm Rennova Cannulas® (Feel Tech Co., Jeollabuk-do, South Coreia) cannulas, with no clogging of the cannulas throughout the procedure for both sides.
After application, massage was performed on the treated areas for approximately 5 minutes. Patients were instructed to massage the treated areas twice a day for 5 minutes for 5 days. Sixty days later, a new treatment session was carried out, with the applications following exactly the same sequence as the first session.
Assessments:
The assessments were carried out at 3 and 6 months after the last application through the following:
Questionnaire applied to patients and the investigator with questions about the perception of
response to treatment. Flaccidity improvement score was assessed according to the Blyumin- Karasik scale (Table 2).8
- Photos of the treated areas in the same positions as in the pre-treatment assessment.
- High-resolution ultrasound examination at 8 points of each arm, through a high-frequency transducer (18 MHz), to observe the skin thickness by the same investigating physician.
| Score | Improvement assessment |
| 0 | 0%: No improvement |
| 1 | 1-25%: Minimal improvement |
| 2 | 26-50%: Moderate improvement |
| 3 | 51-75%: Majorimprovement |
| 4 | 76-100%: Excellent improvement |
Table 2: Assessment of skin flaccidity improvement (Blyumin-Karasik Scale) 8
Statistical analysis:
To analyze the application of Poly-L-Lactic Acid for the treatment of flaccidity in the medial region of the arms, the Shapiro-Wilk test was used in order to test the normality of the data (p>0.05). Then, the ANOVA test was applied for repeated measures using Tukey's post-hoc b test to identify an existing difference between the moments, thus understanding the momentary disparities after acid application.
Finally, they were used as averages of the measurements at each moment to study the behavior of the dermis thickness measurements. For all analyzes, a confidence level of 95% was used. The program used was Stata version 16.0.

*A – Statistical difference with the first moment. B - Statistical difference with the second moment.
Table 1A: Analysis of the mean thickness of the dermis between the moments according to measurements taken on the right arm.

*A – Statistical difference with the first moment. B - Statistical difference with the second moment.
Table 1B. Analysis of the mean thickness of the dermis between the moments according to measurements taken on the right arm.

*A – Statistical difference with the first moment. B - Statistical difference with the second moment.
Table 2A: Analysis of the mean thickness of the dermis between the moments according to measurements taken on the left arm .

*A – Statistical difference with the first moment. B - Statistical difference with the second moment.
Table 2B. Analysis of the mean thickness of the dermis between the moments according to measurements taken on the left arm .
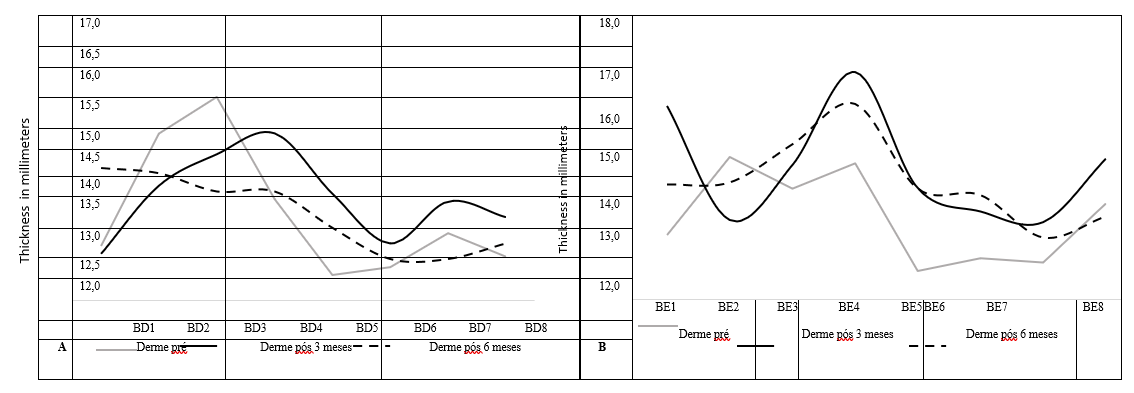
Figure 7: Panel for measuring the thickness of the dermis performed on the upper limbs (A – Right arm, B – Left arm) according to pre, post 3 months and post 6 months
Results:
Four women aged 18 to 64 years (mean age of 45 years) were treated with complaints of skin flaccidity in the medial region of the arms, being the left side treated with RE and the right with the comparator product. Age (based on years), the arm in which the application was performed (right or left), baseline results (pre-application) and after 3 and 6 months of treatment were evaluated, the results are shown in Table 3.
| Patient ID | Age in years | Application site | Pre- application | After 3 months | After 6 months |
SMC | 18 | R arm | Grade2 | Grade1 | Grade1 |
L arm | Grade2 | Grade1 | Grade1 | ||
LB | 45 | R arm | Grade3 | Grade2 | Grade2 |
L arm | Grade3 | Grade1 | Grade1 | ||
VMC | 56 | R arm | Grade3 | Grade2 | Grade2 |
L arm | Grade3 | Grade1 | Grade1 | ||
MC | 64 | R arm | Grade3 | Grade2 | Grade2 |
L arm | Grade3 | Grade2 | Grade2 |
Table 3: Score of the degree of flaccidity of the inner part of the arms in the perception of the patients, according to the SLSS scale of Blyumin-Karasik et al, in the pre-treatment periods, after 3 months and after 6 months of the second application. * R arm: right arm; * L arm.
When performing the tweezers movement to show the flaccidity in the arm of a patient treated with the comparator product, it is demonstrated that after 6 months, visually, it was not possible to observe great decreases in the flaccidity of the arm (Figure 2). This demonstrates that even in the period of 6 months after the applications, with the naked eye, no major changes in the patient's sagging were demonstrated.
The evaluation of the arm treated with Rennova Elleva® was performed and demonstrated that the comparison between before and after 6 months of application (Figure 3A and Figure 3B), it was possible to observe with the naked eye, improvement in the result and a notable decrease in the flaccidity of the patient's arm (Figure 3C and Figure 3D).
The degree of sagging of the arms was evaluated by comparing the result before the application (baseline), 3 months after and 6 months after. Although it was not possible to observe a statistical difference between the groups or between the periods evaluated due to the reduced number of participants, it was possible to observe a greater reduction tendency of the SLSS mean scale in RE treatment (54%, p=0.12), when compared to the comparator product (36%, p=0.88), after 3 and 6 months of application (Figure 4).
An evaluation carried out 3 months after the application of the products showed that the epidermal-dermal thickness (in centimeters) increased significantly in the regions where RE was applied. Added to this, 6 months after application, Rennova Elleva® still performed better when compared to the comparator product. In contrast, the comparator product treatment was not able to change epidermal-dermal thickness at both 3 and 6 months. The statistical evaluation carried out in order to compare the results of the products, at 3 and 6 months after the first application, demonstrated that Rennova Elleva® is statistically significant in the improvement of the epidermal- dermal thickness (p<0>0.05) (Figure 5).
The ultrasound examination, a higher percentage of improvement was also observed on the left side treated with Rennova Elleva® in two patients, perhaps related to the greater and more homogeneous dispersion of its particles when compared to those of the comparator product (Figure 6). [16-17].
Discussion:
PLLA is an injectable synthetic polymer from the alpha-hydroxy-acids family, being biocompatible and biodegradable, with very low cytotoxicity, and used for many years in absorbable sutures. Once injected, PLLA promotes a subclinical local inflammatory response shortly after application, recruiting monocytes, macrophages, and fibroblasts. New collagen begins to form one month later and continues to build up over a period of nine months to one year. In the sixth month, many particles become porous and surrounded by macrophages. PLLA is then hydrolyzed into lactic acid monomers and eliminated, leaving the increased collagen deposition produced by fibroblasts with subsequent increase in dermal thickness.
This fibroplasia will determine the cosmetic results, increasing the tissue volume in a gradual and progressive way, leading to the recovery of the collagen network and improvement of skin flaccidity over the months. [2.4-6]. Its mechanism of action has key implications for the way the product should be applied, how to increase its results, and how to avoid adverse effects.
As results may not be evident for weeks after application, it is crucial to wait for the biological response to occur between each application, with applications of additional treatments being made with an interval of at least 4 weeks. [4,5]. The articles recommend 2 to 4 applications with intervals of 30 to 60 days.[14].
The response time and the degree of improvement in the correction depend essentially on the individual response of each patient, which in turn may vary according to age, sex, skin quality, phototype, and diet. Each application in the treatment with PLLA leads to collagen formation, whose magnitude also depends on the concentration and volume used. [14,15].
Therefore, a choice was made for two applications with intervals of 60 days between them as well as assessments caried out in the pre-treatment period, after three months and after six months of the second application. Both PLLA microparticle presentations were applied to the same patient and to the same area of the arms, so that differences determined by individual or external factors, which may interfere in the therapeutic response, could be eliminated during this study.
However, when we compare the two substances, the different result is remarkable, according to table 2A and 2B. The comparison table shows the superiority of Rennova Elleva®.
We can observe especially in the SM patient an extremely significant improvement in time 3 of his measurements in relation to the comparator product. To better present the general gradual improvement of Rennova Elleva® applications, we checked the graph in the line after 6 months.
Analyzing these results, we can raise the hypothesis that the Rennova Elleva® formulation shows signs of being more effective in its action than that of the comparator.
In the graph shown, we can see, it starts with a peak of improvement in the line after 6 months of approximately 16mm for a stability of 14mm. In the comparator, we can see that the initial peak is 15mm but there is only a decline ending at 13mm.
The Rennova Elleva® molecule shows superior comparator stability with respect to loss of short-term dermal thickness response. This must be confirmed in a protocol with a larger number of patients and for a longer period, but these are encouraging results for other studies.
However, the responses in this case report are very relevant and provide sufficient grounds for a next phase of a randomized project, where we will be able to assess safety and efficacy with a higher patient’s number.
As highlighted in the studies on PLLA,[5]. the adverse reactions reported by patients included pain and bruising by all patients. The pain was mild and did not interfere with the follow- up of the study. As for hematomas, an interesting finding is the decrease in their appearance in the second application for 100% of patients, which may correspond to an improvement in vascular fragility at the treated site. There were no cases of early nodule formation or late granuloma formation during the period evaluated.
Therefore, the two presentations containing PLLA microparticles demonstrated efficacy and excellent therapeutic response, with a slight superiority of the left side treated with Rennova Elleva® according to the patients’ assessment and ultrasonographic measurements, with few adverse effects.
Conclusion:
The application of PLLA to improve sagging facial and body skin is already well known. In this study, the clinical response and the increase in dermal thickness were compared between two presentations of PLLA applied with subdermal injections in the inner region of the arms. The results showed that there was a statistically significant increase in the epidermal-dermal thickness where Rennova Elleva® was applied. On the other hand, the comparator productshowed no improvement in sagging, as well as epidermal-dermal thickness. It is suggested that for future studies, a larger number of patients be used.
Rennova Elleva® through its moleculares model shows promise. In view of the results obtained, it is necessary to expand this pilot project to a project with a larger number of the patients in a randomized study, where we will have a greater dimension of its superiority and a more robust record of its safety and effectiveness. Evidently, we take into account the variables that may occur, since the patient's cooperation after the application is necessary, but the result was promising.
In order to measure Rennova Elleva's superiority, we considered the average of values pre and post 6 months of application.
We can observe an isolated case of higher percentage reaching a total of 16.95% compared to 2.34% of the comparator product. The results are promising, because despite the small number of patients analyzed, we can see that out of the 4 patients, 3 had better results than the comparator product.
To verify its effectiveness and superiority, we will increase the number of the patients in a randomized project to better measure these results.
Disclosure:
The author reports no conflicts of interest in this work
References
- Yaar M, Gilchrest B. (2008). Aging of skin. In: Fitzpatrick’s Dermatology in General medicine. 7th ed. New York: McGraw-Hill Medical, c2008. p. 963-973.
View at Publisher | View at Google Scholar - Cunha MG et. al. (2016). Poly-L-lactic acid injections in sagging body skin. Surg Cosmet Dermatol;8(4)322-327.
View at Publisher | View at Google Scholar - Haddad A, Cunha MG et al. (2019). Recommendations on the Use of Injectable Poly-L- Lactic Acid for Skin Laxity in Off-Face Areas. J Drugs Dermatol; 18(9):217- 223.
View at Publisher | View at Google Scholar - da Cunha MG et al. (2020). Biostimulators and their mechanisms of action. Surg Cosmet Dermatol. 12(2):109-117.
View at Publisher | View at Google Scholar - Machado Filho CDS, Santos TC, Rodrigues APLJR, Cunha MG. (2013). Ácido Poli-L- Láctico: um agente bioestimulador. Surg Cosmet Dermatol; 5(4):345-350.
View at Publisher | View at Google Scholar - Avelar LE, Cazerta C. (2018). The improvement of the skin quality with the use of PLLA. J Dermat Cosmetol;2(2):110–111.
View at Publisher | View at Google Scholar - (2022). Innovapharma. Bula Rennova Elleva® [Internet]. Injectable Poly-L-Lactico Acid Powder.
View at Publisher | View at Google Scholar - Blyumin-Karasik M et al. (2011). Skin tightening of aging upper arms using an infrared light device. Dermatol Surg. 2011 Apr;37(4):441-449.
View at Publisher | View at Google Scholar - Levy J et al. (2021). High-frequency ultrasound in clinical dermatology: a review. Ultrasound J;13(1):24.
View at Publisher | View at Google Scholar - Bhatta AK et al. (2018). Application of high frequency ultrasound in dermatology. Review. Discov Med; 26(145):237-242.
View at Publisher | View at Google Scholar - Al-Himdani S, Ud-Din S, Gilmore S, Bayat A. (2014). Striae distensae: a comprehensive review and evidence-based evaluation of prophylaxis and treatment. Br J Dermatol. 2014; 170(3):527-547.
View at Publisher | View at Google Scholar - da Cunha MG et al. (2017). Anatomical, Histological and Metabolic Differences Between Hypodermis and Subcutaneous Adipose Tissue. Int Arch Med - Section: Dermatology; 10(152):1-6.
View at Publisher | View at Google Scholar - Carneiro JL, Cunha MG et al. (2020). The effects of estrogens and phytoestrogens on human skin and its topical use for prevention of skin aging - Literature Review. Surg Cosmet Dermatol. 2020; 12(1): 11-15.
View at Publisher | View at Google Scholar
