

Review ariticle | DOI: https://doi.org/10.31579/2835-7957/087
Cigarette Smoking as a Hazard Figure for Tuberculosis in Grown-ups: The study of disease transmission and Angles of Infection Pathogenesis
Thank God Onuoha, Biological Sciences Department, Novena University, Ogume, Delta State, Nigeria.
*Corresponding Author: Thank God Onuoha, Biological Sciences Department, Novena University, Ogume, Delta State, Nigeria.
Citation: Thank G. Onuoha (2024), Cigarette Smoking as a Hazard Figure for Tuberculosis in Grown-ups: The study of disease transmission and Angles of Infection Pathogenesis, Clinical Reviews and Case Reports, 3(5); DOI:10.31579/2835-7957/087
Copyright: © 2024, Thank God Onuoha. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 May 2024 | Accepted: 17 June 2024 | Published: 01 July 2024
Keywords: antibiotic resistance; biofilm; mycobacterium tuberculosis; nicotine; smoking
Abstract
The World Health Organization found that there were 10. 6 million people with tuberculosis in the world in 2022. This led to 1. 3 million deaths. Tuberculosis is one of the most widespread and deadly infectious diseases worldwide. Since 1918, people have been arguing about whether smoking cigarettes is connected to TB. Many studies have shown that smoking, whether you do it yourself or breathe in smoke from others, increase the risk of getting tuberculosis and makes the disease worse. With this entire evidence showing that smoking is linked to TB, it is not surprising that TB control programs are an important way to prevent it. The article talks about how TB is linked to smoking and how it spreads. It also discusses studies about how the body fights the TB bacteria. This includes looking at the role of alveolar macrophages in defending against the TB bacteria. Tuberculosis is a serious infection caused by bacteria that can make people very sick. Next, the review will discuss the main ways the germ uses to get around the body's defenses in the airway. This is made worse by the effects of smoke on the lungs' ability to fight off the germ. Lastly, how smoking can make bacteria more resistant to antibiotics because of the direct impact of smoke on the bacteria was looked at. Some bacteria form a slimy layer, pump out harmful substances, and change their genes to resist antibiotics.
Introduction
The WHO says that in 2022, about 10. 6 million people got sick with tuberculosis (TB) around the world, and 1. 3 million people died from it. In 2019, a study found that 1 in 4 people worldwide have latent tuberculosis infection. In many places, including South Africa where TB is common, a lot of people with TB smoke and drink alcohol a lot(2,3, 5). Since 1918, people have been arguing about whether smoking cigarettes is connected to TB. An article in 2010 said that many studies have shown that smoking, whether it's done actively or if you breathe in smoke from others, increases the risk of getting tuberculosis (9, 10, 12). It also makes the disease more dangerous and increases the chances of dying from it (13, 14,16). While we know there are a few studies that say smoking might be linked to some tuberculosis problems, these studies are mostly influenced by other factors. There is a lot of evidence that shows smoking are linked to TB. Because of this, it's suggested that TB control programs should start including ways to help people stop smoking. This review looked at books and articles that talked about how smoking can cause tuberculosis. This is about how alveolar macrophages get rid of Mycobacterium tuberculosis germs in the lungs and how the germs fight back. It also talks about how smoking can weaken the body's ability to fight the germs. Finally, the smoke has direct effects on M. tuberculosis itself, which helps the germ stay in the airways, is talked about briefly [17,18,19, 20].
Study of Smoking and Tuberculosis
Many old studies have shown that smoking is linked to TB in different places. In a study, it was found that people who have smoked in the past, currently smoke, or have ever smoked are more likely to get TB compared to people who have never smoked. The chance of getting TB depends on how much and how often someone smokes, and for how long, and what kind of tobacco they use. In many studies, it was found that smoking a lot for a long time is related to getting TB (21, 22, 23). But not all studies showed this. In a study of older people in Hong Kong, researchers found that the more someone was exposed to TB, the more likely they were to get sick with it (20). Also, a study found that smoking is related to how TB shows up in the body and how it responds to treatment. The study suggests that smoking could cause TB. Another study found that smoking increases the risk of getting TB and getting sick from it. But it's not clear if smoking makes it more likely for people with TB to die. Even young people who smoke are more likely to get TB in their lungs. The more cigarettes they smoke each day, the higher their risk. [19] So, most of the early research showed that there was a strong connection between smoking and TB. This research didn't specifically look at the risk of going from being exposed to TB to being infected, and then from being infected to developing the disease (29).
Breathing in other people's cigarette smoke
The research shows that being around secondhand smoke can also increase the risk of getting TB. For instance, a study showed that children who breathed in tobacco smoke were more likely to get lung TB right after getting infected [21]. Kids between 0-4 years old and 5-9 years old had a higher chance of something bad happening compared to kids who were 10 years old or older. The more cigarettes adults in the household smoked each day, the more likely they were to get TB. This was especially true right after being infected. Two research studies and a combined analysis of data also showed that being around secondhand smoke is linked to developing tuberculosis disease. In one study, the authors found that smoking cigarettes increased the risk of getting TB. Smokers were more likely to have a positive TB test and to get sick and die from TB. Also, being around people who smoke can also make you more likely to get TB, but the evidence for this is not as strong. Leung and others It was found that breathing in smoke from others can increase the risk of getting tuberculosis. This was shown in a study that took into account other factors that could affect the results (21).
Other ways to breathe in smoke
It has been observed that smoking marijuana, inhaling biomass fuel smoke, using marijuana, being exposed to traffic air pollution could increase the risk of getting tuberculosis (1,2, 3). Cigarette smoking makes it harder to diagnose TB. In a new study, it was found that smoking is linked to patients taking longer to get diagnosed. Other studies have also shown that smoking causes delays in both patients and the health system. We don't know all the reasons for why the diagnosis was delayed, but one reason could be that coughing due to tuberculosis was mistaken for coughing from smoking. Delaying in finding out what's wrong can lead to more serious illness, more problems, longer time being able to spread the illness, more deaths, stronger drugs being needed, more people needing to go to the hospital, and more money being spent on healthcare [5,6, 7].
The effects of smoking amongst TB patients.
Smoking makes TB worse, and smokers have more signs and symptoms of pulmonary TB. In a study, it was found that smokers were 1. 5 times more likely to develop lung disease, 1. 9 times more likely to develop cavitary lung disease, and 1. 8 times more likely to need to go to the hospital for a longer period of time. So, in that study, it was found that smoking made TB get worse more quickly and more severely. Furthermore, the cost of hospital stays for people with TB goes up by about EUR 1,000,000 each year. Many other scientists have talked about how smoking makes lung problems worse. It can cause more serious lung damage and holes in the lungs [29].
The effects of smoking on when and how long it takes for cultures to test positive.
Research has found that people who smoke tend to have more positive test results for harmful bacteria at the beginning of the study. A study compared people who smoke with those who don't, and found that people who used to have TB are 1. 36 times more likely to have TB again if they smoke. A new study found more tuberculosis germs in spit. This was found in another research study that people who smoke have more TB bacteria in their spit, making it harder for them to get better. Studies also show that smoking can make it take longer for TB tests to show that someone is not contagious. In a study, it was found that the time it takes to get rid of the TB bacteria from the body is longer for people who smoke more. Smoking more than 20 cigarettes a day can make it 11. 6 times more likely to have the bacteria in the body for a longer time. This is concerning because it means that the person can spread the illness to others for a longer time [17, 18, 19].
Unsuccessful treatment and results of TB treatment in people who smoke.
Smoking and getting older make it more likely for TB treatment to not work well. Even after taking age into account, patients who have smoked in the past still have a higher risk (a 1. 1 to 41 times higher risk) compared to those who have never smoked. In another research, smoking made it harder for treatment to work well (OR = 0. 76; 95% CI 0. 69 to 084; p < 0>
Programs to control tobacco are very important for controlling tuberculosis.
Because cigarette smoking has a big effect on TB disease, researchers have been saying for a long time that it's really important to help people quit smoking in order to control TB as part of TB control programs. Unfortunately, some studies have shown that in certain places, doctors didn't know much about how to help people quit smoking. In these areas, doctors need to learn more about how to help people stop smoking and make it part of their treatment for tuberculosis. Healthcare workers find it hard to help people quit smoking because they are very busy and don't have much time with each patient (4, 27,28). There are also other factors like how people think about smoking and how it affects society that need to be dealt with. Research on healthcare workers has shown that efforts to help people quit smoking should happen not only in hospitals and clinics, but also in the community. This should involve working with the media and families, and addressing healthcare obstacles to make sure these efforts work well [7,8, 10]. A study checked on Chinese TB patients 5 years after they got help to quit smoking. It found that non-smokers, ex-smokers, and current smokers who got help were more likely to still not smoke than those who didn't get help. The authors found that TB program managers should make sure that they include advice on how to quit smoking and have a policy against smoking in TB services. A study about math and smoking said that if people kept smoking the way they were, there would be more TB cases and deaths. But if they made strict rules about smoking, it could save many lives from TB. This part of the article mostly talked about cigarette smoking, but it's also important to think about cutting down on other types of smoking, breathing in smoke from burning wood, using e-cigarettes, and breathing in pollution from cars. Doing this would probably help to decrease the negative effects on how TB develops, how serious it gets, and what happens in the end. Important topics discussed in the previous sections are listed in Table 1.
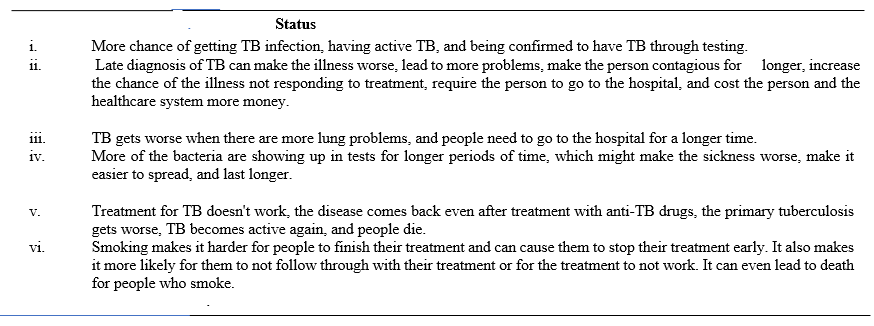
Table 1: Cigarette smoking effects on tuberculosis (TB) patients.
Some people think that being around secondhand smoke, using marijuana, breathing in smoke from cooking fires inside, and being in areas with a lot of traffic could make the health problems of TB patients worse. The information in this table comes from the articles that are mentioned [5,16,19,27]. As portrayed within areas of this survey, cigarette smoking speaks to a well-recognised and inauspicious chance figure for the advancement of TB, which is compounded by the anti-microbial versatility of M. tuberculosis (5). The components used by this pathogen to demolish the intrinsic and versatile defensive safe instruments of the human respiratory tracts, increased by the immunosuppressive impacts of inward breath of tobacco smoke, have been the subject of a few later comprehensive, enlightening reviews (5,7, 11, 13,14). Taking this under consideration, the remaining segments of the current audit are centered particularly on upgrading the components by which the pathogen accomplices with smoking to demolish the anti-mycobacterial exercises of the alveolar macrophage, counting the key inclusion of nicotine in empowering intracellular bacterial survival, perseverance, and expansion, coming about in improvement of aspiratory TB. This approach requires an diagram of the anti-mycobacterial components of alveolar macrophages.
Initial Habitation of M. tuberculosis in the Respiratory Tract
Humans get sick when they breathe in tiny droplets of M. The body normally fights off tuberculosis germs with the help of the respiratory system. However, in smokers, the body's ability to protect the lungs is weakened because the toxic substances in tobacco smoke harm the cilia in the respiratory system. This causes the lungs to produce thick and sticky mucus, and the cilia move slower and not in sync. Once the pathogen escapes the body's initial defenses against smoke and moves to the next important stage in causing disease, it finds a safe place in the alveolar macrophage, which is its main cell host. Living in this area, M .tuberculosis has different ways to survive and grow inside cells, as explained before. Research shows that airway immune cells can be affected by exposure to cigarette smoke [17, 25, 26,27].
How Alveolar Macrophages Fight Against Mycobacteria
Mycobacterium tuberculosis has many different patterns that can make people sick, and some of these patterns help it stick to and invade cells. This helps the immune system recognize and absorb the germ inside phagosomes by interacting with receptors on immune cells in the lungs. These include: (i) Toll-like receptor 2 (TLR2) in different forms, and TLR4; (ii) scavenger receptors like CD36, SRA, MARCO, and several other C-type lectin receptors; and (iii) CD14, which interacts with lipopolysaccharide. Other receptors on alveolar macrophages include CR1, CR3 and CD43. They bind to different things like C3b, Cpn and mycobacterial fimbriae. Mycobacterium tuberculosis is a type of bacteria that can cause infections in people with weak immune systems. The phagosome that contains tuberculosis goes through a process where it gets stronger and can fight the tuberculosis better. The process of phagosome maturation requires certain proteins and lipids to come together and form a phagolysosome, which is a type of organelle that has enzymes to fight off germs. When the process of maturation is finished, the pH level decreases inside the phagolysosome to around 4-5(9). This is because a certain enzyme called vacuolar H+-ATPase is brought in to help with this. This creates a bad environment for germs with substances that can kill bacteria, like oxygen and nitrogen compounds, and enzymes that break down germs [10, 11,12].
LC3-related Phagocytosis
LC3-associated phagocytosis is another way that macrophages get rid of M cells inside the body. Tuberculosis is a disease that affects the lungs [13]. This process uses autophagy and NADPH oxidase to create special membranes called laposomes. After enzymes and ROS modify LC3, mature laposomes combine with lysosomes to make phagolysosomes. This event helps to kill bacteria using ROS made by NOX2. This happens in two ways: first, by making the environment inside the bacteria-eating cells more acidic, and second, by changing the structure of the cell membranes to make them more stable. Described below is M. tuberculosis has many ways to stop the maturation and acidification of phagosomes and lysosomes, and to prevent them from fusing with the pathogen-containing structures. To outsmart the pathogens that try to hide inside cells, macrophages have come up with a different way to kill bacteria called "autophagy". In this process, the membrane of the dysfunctional phagosome is made permeable by a system called ESX-1, which is used by a bacterium called M. tuberculosis and the power of a protein called ESAT-6 to break through membranes. This causes the movement of bacterial DNA to the inside of the cell and makes it visible to a protein called STING. This happens before the pathogen gets ubiquitinated. These happening makes M. Tuberculosis recognized by certain proteins in the body, which then grab the bacteria and bring them to a part of the cell that gets rid of them. This helps the body fight off the tuberculosis bacteria [27]. Autophagosomes come from phagophores. These are structures with two layers that stretch to take in things, and then close to make a sealed autophagosome. Xenophagy is a process where cells capture and break down damaged phagosomes containing M. Tuberculosis. This is when the cytoplasmic galectin is bonded. This attracts autophagy receptors like NDP52, CALCOCO2, and TRIM proteins. These proteins bind to LC3 and move contents to autophagosomes [29]. They also help to join lysosomes together killing bacteria inside cells. Tuberculosis happens because the body changes how it uses energy in immune cells called macrophages. Instead of using their usual way of making energy, they start using a different way called aerobic glycolysis [30]. In this situation, special cells in the lungs called alveolar macrophages change from being less active to becoming more inflammatory and using sugar for energy. These cells were taken from fluid in the lungs. This process is caused by low oxygen levels and turns on genes that make glucose transporters and enzymes that help break down glucose. This change in metabolism happens when mycobacteria molecules and lung cells interact. It also activates a process that releases certain substances in the body. Also, the way the glycolytic enzymes work together not only helps provide the energy needed to move protons across the vacuolar membrane, but also helps keep this complex stable[2, 14 ,16].
Ways Used by M. tuberculosis weakens the body's ability to fight germs.
Tuberculosis bacteria use different proteins and fats to avoid being eaten by the macrophages and to stop the vacuoles from getting rid of them. This makes it hard for the body to get rid of the bacteria. These M examples are very important. Tuberculosis can survive in the body in the following ways:
i . Reduced ability to clean up harmful substances because certain genes are not working properly, but we don't know exactly how this happens [85]. Also, a protein called CpsA has been found to stop the process of LC3-associated phagocytosis and bacterial killing by preventing NOX2 from being recruited to the cells that surround bacteria.
ii. Disruption of the creation of vacuoles, the process of phagosome maturation, and the formation of phagolysosomes is caused by different methods that either activate or work against a substance called phosphatidylinositol-3-phosphate (PI3P). These methods include PI3P secretory acid phosphatase (SapM), PI mannoside, and mannose-capped lipoarabinomannan, as well as the deactivation of small Rab GTPases by mycobacterial nucleoside diphosphate kinase (Ndk) [10, 12, 15].
iii. Mycobacterial protein tyrosine phosphatase A (MptpA) blocks the vacuolar H+-ATPase. Experimentally infected murine bone marrow-derived macrophages and human alveolar macrophages were found to produce more microRNA-21 (miR-21). Tuberculosis might be caused by how the germ interacts with TLR4. This can lower both glycolysis and expression of IL-1β. MiR-21 stops glycolysis by reducing the activity of an enzyme called phosphofructokinase. SLS and DIMs have been found to be important in stopping autophagy caused by mycobacteria. In one situation, blocking the process of autophagy was connected to reducing the activity of certain immune cells in the lungs. In another situation, certain compounds were seen to reduce the acidity of compartments that contain harmful pathogens. Also, a type of molecule found in mycobacterium bacteria called 1-tuberculosinyladnosine has been shown to stop the normal process of cells maturing and blocking the process of autophagy (11). This causes a change in the type of cells in the immune system from one that fights infection to one that stores fat, which is a key feature of tuberculosis as shown in table 2 below.
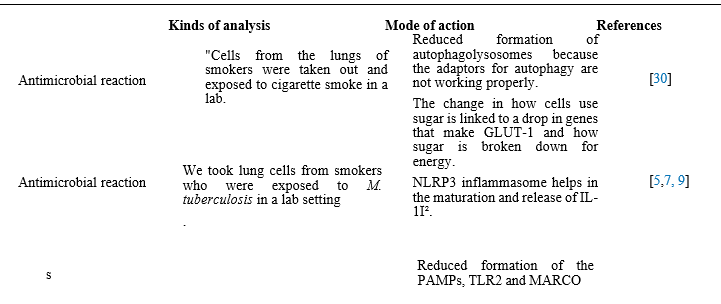
Table 2: How smoking and nicotine can weaken the immune system in the lungs.
Key: nAChR—nicotinic acetylcholine receptor; GLUT1—glucose transporter 1; MARCO—macrophage receptor with a collagenous structure; IL-1β—interleukin-1β; NFκB—nuclear factor kappa B; NLRP3 inflammasome—(nucleotide-binding domain, leucine-rich-containing family, pyrin domain-containing-3) in- flammasome; miRNA—micro ribonucleic acid; PAMPs—pathogen-associated molecular patterns; STAT3—signal transducer and activation of transcription 3; TLR2—Toll-like receptor 2; Tregs—regulatory T cells.
Conclusion
Smokers are at greater risk of getting very bad TB that doesn't respond to medicine. This is a big problem in many countries, especially in poorer ones. Many people don't want to quit smoking, and big tobacco companies make it worse by advertising to young people in poor countries. Despite there being a lot of evidence from studying diseases in large groups of people, we have also learned a lot from studying individual patients and doing experiments in the lab. We have found out how smoking makes tuberculosis worse in many different ways, including by harming the immune cells in the lungs and by directly hurting the TB bacteria. In the first case, this happens by weakening the pathways inside cells that are involved in getting rid of M. tuberculosis can become stronger by changing its genes to resist antibiotics and by forming a protective layer. Another worry is that nicotine might make it harder for the body to fight off bacteria. This raises questions about whether nicotine replacement products are actually helpful in preventing illness from bacteria. Tuberculosis is a contagious disease caused by bacteria that usually affects the lungs. Therefore, it is imperative for smokers especially do suffering from TB to quit smoking so as to avoid resistance of M. tuberculosis to medication.
References
- Cohen, A.; Mathiasen, V.D.; Schön, T.; Wejse, C. (2019). The global prevalence of latent tuberculosis: A systematic review and meta- analysis. Eur. Respir. J., 54, 1900655. [CrossRef] [PubMed]
View at Publisher | View at Google Scholar - Wessels, J.; Walsh, C.M.; Nel, M. (2019). Smoking habits and alcohol use of patients with tuberculosis at Standerton Tuberculosis Specialised Hospital, Mpumalanga, South Africa. Health SA, 24, 1146. [CrossRef] [PubMed]
View at Publisher | View at Google Scholar - Webb, G.B. (2024). The effect of the inhalation of cigarette smoke on the lungs. A clinical study. Am. Rev. Tuberc. 1918, 2, 25–27. Available online: https://www.atsjournals.org/doi/epdf/10.1164/art.1918.2.1.25 (accessed on 5 January 2024).
View at Publisher | View at Google Scholar - Chan, E.D.; Keane, J.; Iseman, M.D. (2010). Should cigarette smoke exposure be a criterion to treat latent tuberculous infection? Am. J. Respir. Crit. Care Med. 182, 990–992. [CrossRef] [PubMed]
View at Publisher | View at Google Scholar - Bay, J.G.; Patsche, C.B.; Svendsen, N.M.; Gomes, V.F.; Rudolf, F.et al. (2022). Tobacco smoking impact on tuberculosis treatment outcome: An observational study from West Africa. Int. J. Infect. Dis., 124, S50–S55. [CrossRef]
View at Publisher | View at Google Scholar - Gambhir, H.S.; Kaushik, R.M.; Kaushik, R.; Sindhwani, G. (2010). Tobacco smoking-associated risk for tuberculosis: A case-control study.
View at Publisher | View at Google Scholar - Int. Health (2010), 2, 216–222. [CrossRef]
View at Publisher | View at Google Scholar - Pai, M.; Mohan, A.; Dheda, K.; Leung, C.C.; Yew. Et al. (2007). Lethal interaction: The colliding epidemics of tobacco and tuberculosis. Expert Rev. Anti Infect. Ther.5, 385–391. [CrossRef]
View at Publisher | View at Google Scholar - Kolappan, C.; Gopi, P.G. (2005). Tobacco smoking and pulmonary tuberculosis. Thorax, 57, 964–966. [CrossRef]
View at Publisher | View at Google Scholar - Den Boon, S.; van Lill, S.W.; Borgdorff, M.W.; Verver, S.et al. (2005). Association between smoking and tuberculosis infection: A population survey in a high tuberculosis incidence area. Thorax, 60, 555–557. [CrossRef]
View at Publisher | View at Google Scholar - Hassmiller, K.M. (2006). The association between smoking and tuberculosis. Salud Publica Mex., 48, S201–S216. [CrossRef]
View at Publisher | View at Google Scholar - Slama, K.; Chiang, C.Y.; Enarson, D.A.; Hassmiller, K.; Fanning, A. et al. (2007). Tobacco and tuberculosis: A qualitative systematic review and meta-analysis. Int. J. Tuberc. Lung Dis., 11, 1049–1061.
View at Publisher | View at Google Scholar - Alavi, S.M.; Ershadian, S. (2003). Association between cigarette smoking and pulmonary tuberculosis. Pak. J. Med. Sci. 2009, 25, 912–915. Available online: https://www.pjms.com.pk/issues/octdec209/pdf/08.article07.pdf (accessed on 17 October 2023).
View at Publisher | View at Google Scholar - Alavi-Naini, R.; Sharifi-Mood, B.; Metanat, M. (2012). Association between tuberculosis and smoking. Int. J. High Risk Behav. Addict., 1, 71–74. [CrossRef] [PubMed]
View at Publisher | View at Google Scholar - Bishwakarma, R.; Kinney, W.H.; Honda, J.R.; Mya, J.; Strand, M.J. et al. Chan, E.D. Epidemiologic link between tuberculosis and cigarette/biomass smoke exposure: Limitations despite the vast literature. Respirology (2015), 20, 556–568. [CrossRef] [PubMed]
View at Publisher | View at Google Scholar - Smith, G.S.; Van Den Eeden, S.K.; Baxter, R.; Shan, J.; Van Rie, A.; Herring, A.H.; Richardson, D.B.; Emch, M.; Gammon, M.D. (2015). Cigarette smoking and pulmonary tuberculosis in northern California. J. Epidemiol. Community Health 2015, 69, 568–573. [CrossRef]
View at Publisher | View at Google Scholar - Leung, C.C.; Li, T.; Lam, T.H.; Yew, W.W.; Law, W.S.; Tam, C.M. et al. (2004). Smoking and tuberculosis among the elderly in Hong Kong. Am. J. Respir. Crit Care Med., 170, 1027–1033. [CrossRef]
View at Publisher | View at Google Scholar - Bates, M.N.; Khalakdina, A.; Pai, M.; Chang, L.; Lessa, F.; Smith, K.R. Risk of tuberculosis from exposure to tobacco smoke: A systematic review and meta-analysis. Arch. Intern. Med., 167, 335–342. [CrossRef]
View at Publisher | View at Google Scholar - Alcaide, J.; Altet, M.N.; Plans, P.; Parrón, I.; Folguera, L. et al. (1996). Cigarette smoking as a
View at Publisher | View at Google Scholar - risk factor for tuberculosis in young adults: A case-control study. Tuber. Lung Dis. 1996, 77, 112–116. [CrossRef]
View at Publisher | View at Google Scholar - Chiang, C.Y.; Slama, K.; Enarson, D.A. Associations between tobacco and tuberculosis. Int. J. Tuberc. Lung Dis. 2007, 11, 258–262.
View at Publisher | View at Google Scholar - Altet, M.N.; Alcaide, J.; Plans, P.; Taberner, J.L. et al. (1996). Passive smoking and risk of pulmonary tuberculosis in children immediately following infection. A case-control study. Tuber. Lung Dis. 1996, 77, 537–544. [CrossRef]
View at Publisher | View at Google Scholar - Lin, H.H.; Ezzati, M.; Murray, M. Tobacco smoke, indoor air pollution and tuberculosis: A systematic review and meta-analysis.
View at Publisher | View at Google Scholar - PLoS Med. (2007). 4, e20. [CrossRef]
View at Publisher | View at Google Scholar - Leung, C.C.; Lam, T.H.; Ho, K.S.; Yew, W.W. et al. Passive smoking and tuberculosis. Arch. Intern. Med. ( 2010), 170, 287–292. [CrossRef]
View at Publisher | View at Google Scholar - Tewatia, P.; Kaushik, R.M.; Kaushik, R.; Kumar, S. (2020). Tobacco smoking as a risk factor for tuberculous pleural effusion: A case-control study. Glob. Health Epidemiol. Genom. (2020). 5, e1. [CrossRef]
View at Publisher | View at Google Scholar - Oeltmann, J.E.; Oren, E.; Haddad, M.B.; Lake, L.k.; Harrington, T.A. et al. (2006). Tuberculosis outbreak in marijuana users, Seattle, Washington, 2004. Emerg. Infect. Dis. 12, 1156–1159. [CrossRef] [PubMed]
View at Publisher | View at Google Scholar - Gómez, A.C.; Rodríguez-Fernández, P.; Villar-Hernández, R.; Gibert, I.; Muriel-Moreno, B.; Lacoma, A.; Prat-Aymerich, C.; Domínguez, J. E-cigarettes: Effects in phagocytosis and cytokines response against Mycobacterium
View at Publisher | View at Google Scholar - tuberculosis. PLoS ONE 2020, 15, e0228919. [CrossRef]
View at Publisher | View at Google Scholar - Underner, M.; Perriot, J. Tabac et tuberculose [Smoking and tuberculosis]. Presse Med. (2012). 41, 1171–1180. (In French) [CrossRef]
View at Publisher | View at Google Scholar - Gupta, K.B.; Bansal, A. Delay in diagnosis and treatment of tuberculosis—A review. NTI Bull. (2008). 44, 27–30.
View at Publisher | View at Google Scholar - Basnet, R.; Hinderaker, S.G.; Enarson, D.; Malla, P.; Mørkve, O. Delay in the diagnosis of tuberculosis in Nepal. BMC Public Health 2009, 9, 236. [CrossRef] [PubMed]
View at Publisher | View at Google Scholar - Shu, W.; Chen, W.; Zhu, S.; Hou, Y.; Mei, J. et al. (2014). Factors causing delay of access to tuberculosis diagnosis among new, active tuberculosis patients: A prospective cohort study. Asia Pac. J. Public Health, 26, 33–41. [CrossRef]
View at Publisher | View at Google Scholar - Alavi, S.M.; Bakhtiyariniya, P.; Albagi, A. Factors associated with delay in diagnosis and treatment of pulmonary tuberculosis. Jundishapur J. Microbiol. 2015, 8, e19238. [CrossRef]
View at Publisher | View at Google Scholar
