

Research Article | DOI: https://doi.org/10.31579/2834-5126/150
Challenging Goal Agreement: A Relational and Constructivist Perspective on Therapist–Client Dynamics
- Luísa Soares *
University of Madeira, Portugal.
*Corresponding Author: Luísa Soares., University of Madeira, Portugal.
Citation: Luísa Soares, (2026), Challenging Goal Agreement: A Relational and Constructivist Perspective on Therapist–Client Dynamics, Clinical Trials and Clinical Research,5(5); DOI:10.31579/2834-5126/150
Copyright: © 2026, Luísa Soares. This is an open access article distributed under the creative commons’ attribution license, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 May 2026 | Accepted: 20 May 2026 | Published: 27 May 2026
Keywords: psychotherapy outcomes; therapeutic alliance; goal consensus; treatment dropout; clinical psychology; therapist–client relationship; empathy; client engagement
Abstract
Background:
The therapeutic alliance has been consistently identified as a key factor in psychotherapy outcomes, with goal agreement representing a central component. However, the relationship between therapist–client goal agreement and dropout remains unclear and potentially more complex than traditionally assumed.
Methods:
This study examined therapist–client agreement on therapy goals and its association with dropout in psychotherapy. Thirty-nine therapist–client dyads participated. Therapy goals were assessed using the Goals for Therapy Questionnaire across four sessions (1st, 3rd, 5th, and 8th). Agreement was operationalized based on shared goal categories, and its relationship with dropout was analysed using chi-square tests.
Results:
Findings revealed a fluctuating pattern of agreement and disagreement across sessions. Overall, disagreement between therapists and clients was more frequent than agreement. The relationship between goal agreement and dropout showed a mixed pattern: in some cases, agreement was associated with continuation in therapy, while in others it was linked to dropout. These results suggest that goal agreement alone is not a consistent predictor of therapeutic outcomes.
Conclusion:
The findings highlight the limitations of a purely technical understanding of psychotherapy based on goal alignment. Instead, they support a relational and constructivist perspective, in which differences in goals may reflect distinct meaning-making processes that require ongoing negotiation within the therapeutic relationship. Future research should further explore therapist–client dynamics using process-oriented approaches and larger samples.
Introduction
It is believed that the nature of the relationship between therapist and client predicts, to a large extent, the quality of the therapeutic process and outcome. Indeed, several investigations have shown a positive relationship between the therapeutic relationship and the therapeutic outcome (Baldwin, Wampold, & Imel, 2007; Horvath & Bedi, 2002; Martin, Garske, & Davis, 2000; Norcross, 2002; Schnur & Montgomery, 2010). So, it can be said that the therapeutic relationship, itself, appears to influence more the therapy outcome than the specific therapy ingredients (Norcross, 2002; Shunr & Montgomery, 2010). The construction of therapeutic alliance between therapist and client is undoubtedly considered as a central element of the therapeutic relationship (Baldwin, Wampold, & Imel, 2007; Bordin, 1979; Horvath & Bedi, 2002; Luborsky, 2000; Martin, Garske, & Davis, 2000; Norcross, 2002; Soares et al, 2026). According to Bordin (1979), the therapeutic alliance comprised three components: goals, tasks and bonds. Goals refer to the extend which therapist and client agree on goals for doing therapy. Tasks refers to the extend client and therapist agree on therapy tasks. Bond addresses the sense of attachment between the therapist and client.Beyond the structural components of the therapeutic alliance, recent conceptual developments suggest that the effectiveness of psychotherapy cannot be reduced to technical alignment alone, but rather depends on deeper relational and epistemological processes that shape the therapeutic encounter (Oliveira, Lucas, & Soares, 2026). Evidence has established that goals consensus and collaborative involvement are important factors in determining the quality of psychotherapy outcome (Mackrill, 2010, 2011; Schnur & Montgomery, 2010; Steering Committee, 2002; Tryon & Winograd, 2002). The essence of goal consensus is the therapist-client agreement on therapy goals and the ways to accomplish them (Mackrill, 2010, 2011; Tyron & Winograd, 2002, 2011). In psychotherapy reaching such an agreement is not always easy and immediate (Mackrill, 2011), because too often, clients do not know what they really want to achieve in therapy or the goals they formulated are not sufficiently precise and realistic. In addition, clients’ goals for therapy may include specific goals to their concerns, problems and symptomatology but also broader life goals. Given this great variability, therapists and clients might not share common goals and expectations for therapy (Santos & Soares, 2024). So, in order to minimize possible discrepancies between therapist and client, and to enhance the therapeutic results, the goals for therapy should be analyzed and discussed together (Cooper & Mcleod, 2007; Tyron & Winograd, 2002, 2011). In fact, “psychotherapy is not something done to them but by them” (Mahoney & Granvold, 2004, p. 74). Assuming the importance of these variables for the therapeutic process and its outcome, and the need to continue to understand the complex and unique dynamic established between the therapist and clients, this study aims to analyze the therapist-client agreement on goals and, to see if there is an association between the goal’s agreement for doing therapy and the dropout of clients. In line with contemporary constructivist and integrative perspectives, psychotherapy is increasingly understood as a co-constructed process in which meaning-making and narrative reorganization play a central role in therapeutic change (Santos & Soares, 2024). Furthermore, the classical contributions of Carl Rogers remain highly relevant, particularly regarding the role of unconditional positive regard, genuineness, and empathic understanding as core conditions for effective therapeutic engagement (Soares, Zlochová, & Vyskcilova, 2026).
Method
Participants
Thirty-nine therapist-clients dyads (14 therapists and 39 clients) of the Northern Region of Portugal participated in this study. From the therapists’ sample, thirteen were women and just only one man. The therapist’s age ranged between 27-59 years (M=32.9; SD=8.5). Most therapists were psychologists (92.9 %) and just only one was a psychiatrist (7.1%). Most therapists work in a center for drugs addition (78.6%) in a hospital, school/university and in the clinical setting (21.4%). The problems identified in therapy were: drug addiction (78.6%) and anxiety/depression (21.4%).
From the clients’ sample, 20 were women and 19 were men. The clients’ age was 28.7 and standard deviant 6.9, ranging from 19 to 47 years. For the majority of clients (74%) it was the first time in therapy (74.4%). About 54% of them dropped out from therapy. Of the dropouts, 47% occurred after 1st session, 29?ter 3rd session and 24?ter the 5th session.
Measures
First, we applied a questionnaire to collect demographic data, in order to characterize the sample. Subsequently, we applied the Goals for Therapy Questionnaire, developped by Soares and Lemos (2003), which asses the therapist’ goals and client’s goals for therapy. There are two versions of this questionnaire, one for the therapist and another one for the client. Clients were asked to write down at least three goals they wanted to achieve while doing psychotherapy. On the other hand, therapists were asked to write down at least three goals they wanted achieve with the client during the therapeutic process.
Procedure
The Goal for Therapy Questionnaire was applied at the beginning of sessions 1st, 3rd, 5th and 8th, with the prior informed consent of the participants and the institutions where the therapists works. Participants’ selection was based on their availability to participate in this study. All statistical analyses were performed using SPSS Statistics Program 17.0.
Results
We made a global list of the goals for therapy referred by therapists and by the clients. We also used a non-selective approach, opting to maintain the goals formulated by clients and therapists and grouped them into categories. The final eight categories resulted from an agreement between 2 independent observers. Each observer had previous formulated categories for the goals for therapy mentioned by clients and therapists, and these goals’ categories were share and discussed together. We defined the same categories of goals, for both clients and therapists, to facilitate the statistical analysis. The eight categories of the therapy goals formulated were: (1) self-confidence; (2) problem solving; (3) emotional control; (4) psychological well-being; (5) interpersonal relationship; (6) prevention of drugs consumption; (7) therapeutic support; and (8) academic/professional adaptation. The presence of a common goal by an element of the dyad resulted into a dichotomous variable (0,1), which allowed us to establish the agreement or disagreement in therapist-client dyad regarding the therapy goal category. We considered a goal agreement between therapist and client, when both therapist and client set the same goal category for therapy, in a specific session. On the contrary, when the elements of dyads mentioned different goals for therapy we considered a disagreement. For the statistical analyzes it was excluded the cases where both client and therapist did not mentioned such goal category (e.g., the goal category prevention of drugs consumption was only common in those cases where clients were attending the Center for drug users. In this study, the analysis focus was on the therapist-client agreement in each of the four sessions evaluated of the therapeutic process (1st, 3rd, 5th and 8th) and not throughout the all course of therapy. In order to establish, if there is an association between client-therapist agreement for the therapy goal and the cases that dropout from therapy, it was conducted the chi-square adjustment test. We intend to establish if, the distribution of agreement and disagreement between dyads, in which clients dropped out and those who did not, is the same. Our hypothesis is: the dyads in which clients quit and those who do not, have the same distribution, for p values higher than 0.05 (Schinka, Velicer, & Wayne, 2003). Agreement vs disagreement regarding the goals for therapy. First, we began the analysis of data regarding the frequency of the agreement and the disagreement (see Table 1). In the first session, there were a greater agreement between client and therapist in the following categories of goals: solving problem, emotional control, interpersonal relationship and prevention of drugs consumption. In the third session, the goals’ agreement focused more on problem solving, interpersonal relationship and prevention of drug consumption. We observed that, between the first and third session, dyads basically agreed on the same goals for therapy. Yet, in the fifth session there were more concordance regarding self-confidence, interpersonal relationship and academic/professional adaptation goals’. In the eight session, the number of concordance between therapist and client was higher in self-confidence, prevention of drug consumption and academic/professional adaptation goals’.
Session 1 | Session 3 | Session 5 | Session 8 | ||||||
n | % | n | % | n | % | N | % | ||
Self-confidence | Disagree | 21 | 80.8 | 15 | 75.0 | 6 | 46.2 | 6 | 60.0 |
Agree (Yes) | 5 | 19.2 | 5 | 25.0 | 7 | 53.8 | 4 | 40.0 | |
Problem solving | Disagree | 20 | 64.5 | 11 | 68.8 | 9 | 81.8 | 5 | 62.5 |
Agree (Yes) | 11 | 35.5 | 5 | 31.3 | 2 | 18.2 | 3 | 37.5 | |
Emotional control | Disagree | 10 | 62.5 | 7 | 70.0 | 8 | 80.0 | 4 | 80.0 |
Agree (No) | 6 | 37.5 | 3 | 30.0 | 2 | 20.0 | 1 | 20.0 | |
Psychological well-being | Disagree | 14 | 77.8 | 12 | 75.0 | 8 | 72.7 | 8 | 88.9 |
Agree (No) | 4 | 22.2 | 4 | 25.0 | 3 | 27.3 | 1 | 11.1 | |
Interpersonal relationship | Disagree | 11 | 64.7 | 6 | 50.0 | 6 | 54.5 | 6 | 50.0 |
Agree (Yes) | 6 | 35.3 | 6 | 50.0 | 5 | 45.5 | 6 | 50.0 | |
Prevention of drugs consumption | Disagree | 9 | 60.0 | 4 | 57.1 | 7 | 100.0 | 1 | 50.0 |
Agree (Yes) | 6 | 40.0 | 3 | 42.9 | 0 | 0.0 | 1 | 50.0 | |
Therapeutic support | Disagree | 8 | 80.0 | 6 | 85.7 | 2 | 100.0 | 2 | 66.7 |
Agree (No) | 2 | 20.0 | 1 | 14.3 | 0 | 0.0 | 1 | 33.3 | |
Academic/professional adaptation | Disagree | 12 | 66.7 | 9 | 75.0 | 5 | 55.6 | 4 | 57.1 |
Agree (Yes) | 6 | 33.3 | 3 | 25.0 | 4 | 44.4 | 3 | 42.9 | |
Table 1: Frequencies for session and categories of goals for therapy.
Agreement vs disagreement on therapy goals’ and dropout from therapy. To assess the client and therapist agreement regarding therapy goals’ and the dropouts from therapy, we used the Chi-Square Adjustment test. The results were presented for each category goals.Self-confidence. In the first session (see Table 2), 10% of the dyads who continued the therapy, agreed on self-confidence as a goal for therapy, yet among those who have given up therapy that percentage was 25%. Regarding the goals for the 3rd and 5th session, it was possible to see differences between the two groups (X= 5.143, p<0.05 and X = 6.250, p <0.05). So, in the dyads of clients and therapists that did not give up the therapeutic process, it was higher the number of disagreement, between them, in particular on assuming the self-confidence as a goal for therapy. In the 5th session, this percentage decreased to 55.6%. On the contrary, in dyads in which clients dropped out from therapy, the percentage of agreement was significantly different in the 3rd and 5th session, indicating that the disagreement regarding this goal was related with the permanence in therapy.
| Not give up | Give up | Chi-square adjustment test | ||||
N | % | n | % | X | P | ||
Self-confidence (session 1) | Disagree | 9 | 90.0 | 12 | 75.0 | 2.250 | 0.134 |
Agree (Yes) | 1 | 10.0 | 4 | 25.0 | |||
Self-confidence (session 3) | Disagree | 11 | 84.6 | 4 | 57.1 | 5.143 | 0.023 |
Agree (Yes) | 2 | 15.4 | 3 | 42.9 | |||
Self-confidence (session 5) | Disagree | 5 | 55.6 | 1 | 25.0 | 6.250 | 0.012 |
Agree (Yes) | 4 | 44.4 | 3 | 75.0 | |||
Self-confidence (session 8) | Disagree | 6 | 60.0 | 0 | - | - | - |
Agree (Yes) | 4 | 40.0 | 0 | - | |||
Table 2: Results of Chi-square adjustment test for Self-confidence goal in therapist-client dyads.
Solving problem. In both groups, the percentage of goal agreement was lower, than the percentage of disagreement on this goal (see Table 3).
Not give up | Give up | Chi-square adjustment test | |||||
N | % | n | % | X | P | ||
Problem solving (session 1) | Disagree | 7 | 58.3 | 13 | 68.4 | 2.579 | 0.108 |
Agree (Yes) | 5 | 41.7 | 6 | 31.6 | |||
Problem solving (session 3) | Disagree | 5 | 62.5 | 6 | 75.0 | 0.000 | 1.000 |
Agree (Yes) | 3 | 37.5 | 2 | 25.0 | |||
Problem solving (session 5) | Disagree | 5 | 71.4 | 4 | 100.0 | 2.250 | 0.134 |
Agree (Yes) | 2 | 28.6 | 0 | 0.0 | |||
Problemsolving (session 8) | Disagree | 5 | 62.5 | 0 | - | - | - |
Agree (Yes) | 3 | 37.5 | 0 | - | |||
Table 3: Results of Chi-square adjustment test for Problem Solving goal in therapist-client dyads.
Emotional control. From the sixteen dyads who considered the emotional control, as a goal for doing therapy in the 1st session, ten therapists and clients disagreed that this was a goal shared by them, and six of them had given up therapy in the subsequent sessions. The chi-square adjustment test showed that the percentage of agreement/disagreement was substantially equal, in dyads where clients had quite therapy and those that had not (see Table 4).
Not give up | Give up | Chi-square adjustment test | |||||
n | % | n | % | X | P | ||
Emotional control (session 1) | Disagree | 6 | 66.7 | 4 | 57.1 | 0.571 | 0.450 |
Agree (Yes) | 3 | 33.3 | 3 | 42.9 | |||
Emotional control (session 3) | Disagree | 5 | 71.4 | 2 | 66.7 | 5.333 | 0.021 |
Agree (Yes) | 2 | 28.6 | 1 | 33.3 | |||
Emotional control (session 5) | Disagree | 6 | 75.0 | 2 | 100.0 | 18.000 | 0.000 |
Agree (Yes) | 2 | 25.0 | 0 | 0.0 | |||
Emotional control (session 8) | Disagree | 4 | 80.0 | 0 | - | - | - |
Agree (Yes) | 1 | 20.0 | 0 | - | |||
Table 4: Results of Chi-square adjustment test for Emotional Control goal in therapist-client dyads.
In the 3rd and 5th sessions, we found differences between these two groups of dyads. Therefore, the dyads of clients who dropout from therapy, showed more concordance on goal, than those observed among dyads of clients who remained in therapy. Psychological well-being. Eighteen dyads indicated the psychological well-being as a goal in the 1st session. The distribution was statistically equal, between the dyads who had given up the therapeutic process, and those who had not given up (see Table 5).
Not give up | Give up | Chi-square adjustment test | |||||
n | % | n | % | X | p | ||
Psychological well-being (session 1) | Disagree | 6 | 75.0 | 8 | 80.0 | 0.400 | 0.527 |
Agree (Yes) | 2 | 25.0 | 2 | 20.0 | |||
Psychological well-being (session 3) | Disagree | 7 | 77.8 | 5 | 71.4 | 0.571 | 0.450 |
Agree (Yes) | 2 | 22.2 | 2 | 28.6 | |||
Psychological well-being (session 5) | Disagree | 6 | 75.0 | 2 | 66.7 | 8.333 | 0.004 |
Agree (Yes) | 2 | 25.0 | 1 | 33.3 | |||
Psychological well-being (session 8) | Disagree | 8 | 88.9 | 0 | - | - | - |
Agree (Yes) | 1 | 11.1 | 0 | - | |||
Table 5: Results of Chi-square adjustment test for Psychological Well-being goal in therapist-client dyads.
In sixteen dyads that indicated this goal, in the 3rd session, we observed a good adjustment between the dyads in which clients did not give up therapy when compared to those dyads that clients did. However, we observed significant differences, in eleven dyads that choose this goal in the 5th session, when compared among those who gave up and those who remain in therapy. These differences were explained by the fact that 25% of the dyads agreed that psychological well-being was a goal in this session, while this percentage was 33.3% in dyads who did not end the therapeutic process. Interpersonal Relationship. From thirty-nine dyads in this study, seventeen referred interpersonal relationship as a goal for doing therapy. In six of them, it was observed a concordance between therapist and client regarding this goal category (see Table 6).
Not give up | Give up | Chi-square adjustment test | |||||
N | % | n | % | X | P | ||
Interpersonal relationships (session 1) | Disagree | 6 | 66.7 | 5 | 62.5 | 0.125 | 0.724 |
Agree (Yes) | 3 | 33.3 | 3 | 37.5 | |||
Interpersonal relationships (session 3) | Disagree | 3 | 37.5 | 3 | 75.0 | 4.000 | 0.046 |
Agree (Yes) | 5 | 62.5 | 1 | 25.0 | |||
Interpersonal relationships (session 5) | Disagree | 6 | 54.5 | 0 | - | - | - |
Agree (Yes) | 5 | 45.5 | 0 | - | |||
Interpersonal relationships (session 8) | Disagree | 6 | 50.0 | 0 | - | - | - |
Agree (Yes) | 6 | 50.0 | 0 | - | |||
Table 6: Results of Chi-square adjustment test for Interpersonal Relationship goal in therapist-client dyads.
In three of them, it was observed an agreement between therapist and clients on this goal for doing therapy (p <0.05). When compared with the 3rd session, just twelve dyads referred this as goal category, and in six of them, we registered therapist-client agreement. Additionally, five of these six dyads, did not end prematurely the therapeutic process, and it represented 62.5% of the dyads that remain in therapy versus 25% of dyads in which client gave up therapy. This difference explained the level of significance observed in the Chi-square adjustment test. Prevention of drug consumption. From the thirty-nine dyads, fifteen dyads considered the prevention of drug consumption as a goal in the first session. However, only six dyads had an agreement between the therapist and the client on this goal for therapy. When compared the two groups of dyads, the ones that dropped from therapy and those who remain in therapy, the distribution was statistically equal (see Table 7).
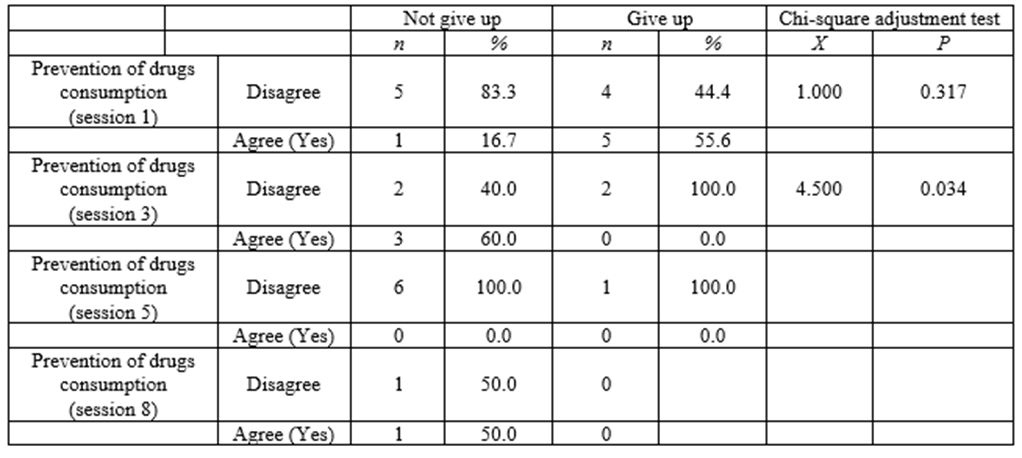
Table 7: Results of Chi-square adjustment test for Prevention of drugs consumption goal in.
In the 3rd session, seven dyads reported this as a goal for doing therapy, but among these, only 3 dyads agreed that the prevention of drugs consumption was a common goal for therapy. Therapeutic Support. Ten dyads reported therapeutic support as a goal in the 1st session. It was also observed an agreement between therapist and client regarding this goal category only in two of them (see Table 8).
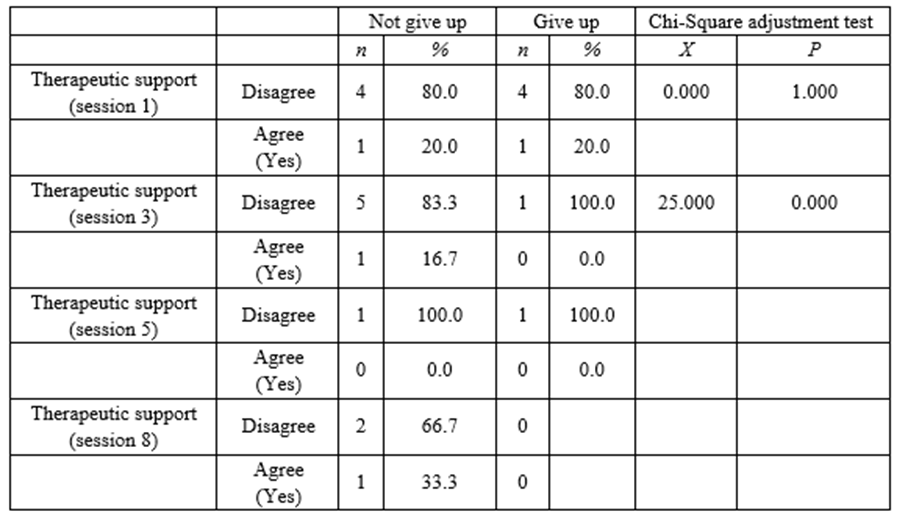
Table 8: Results of Chi-square adjustment test for Emotional Control goal in therapist-client dyads.
There was a perfect adjustment between the two groups, which was not observed in the 3rd session, so the agreement on this goal appears as a promoter for client to remain in the therapy process.
Academic/professional Adaptation. This goal was mentioned in eighteen dyads, and we observed an agreement on such goal in six dyads (see Table 9).
|
| Not give up | Give up | Chi-square adjustment test | |||
n | % | n | % | X | P | ||
Academic/Prof. adaptation (session 1) | Disagree | 6 | 60.0 | 6 | 75.0 | 0.500 | 0.480 |
Agree (Yes) | 4 | 40.0 | 2 | 25.0 | |||
Academic/Prof. adaptation (session 3) | Disagree | 5 | 71.4 | 4 | 80.0 | 0.800 | 0.371 |
Agree (Yes) | 2 | 28.6 | 1 | 20.0 | |||
Academic/Prof. adaptation (session 5) | Disagree | 3 | 50.0 | 2 | 66.7 | 3.000 | 0.083 |
Agree (Yes) | 3 | 50.0 | 1 | 33.3 | |||
Academic/Prof. adaptation (session 8) | Disagree | 4 | 57.1 | 0 | - | - | - |
Agree (Yes) | 3 | 42.9 | 0 | - | |||
Table 9: Results of Chi-square adjustment test for Academic/professional adaptation in therapist-client dyads.
Four of them remained in therapy and two quit therapy. Overall, these results indicated that the effect of client-therapist goal agreement, in each session, had less impact in the 1st session than in the 3rd and 5th sessions.
Discussion
As outlined previously, the main focus of this study was to analyse if clients and therapists tend to agree on goals for therapy and explore its effects on dropouts from therapy. The results showed that therapists and clients did not always share the same goals for therapy in the four sessions evaluated. These findings can be better understood within a constructivist framework, where divergence in goals does not necessarily reflect therapeutic failure, but rather different meaning-making positions that require negotiation and integration
throughout the therapeutic process (Santos & Soares, 2024). The percentage of disagreement on goals for therapy, between therapists and clients were higher than the percentage of agreement. This seems to be in line with some empirical studies of therapist-clients dyads (e.g., Fitzpatrick, Iwakabe, &
Stalikas, 2005; Swift & Callahan, 2009; Soares et al, 2013; Oliveira et al 2026) that found that convergence in goals for therapy does not always occur between therapists and clients. This evidence needs to be discussed among therapists communities. Are we working together, on the same pathway when we engage in a psychotherapy process with our client? Or are we serving just as a hearing audience to his problems? From the eight categories of goals for doing therapy analysed in this study, the goals that clients and therapists seemed to show greater agreement were interpersonal relationship and prevention of drug consumption, since these goals categories were mentioned in all four sessions evaluated. The standard categories of goals for therapy, set by therapists and clients, were more similar in 1st and 3rd sessions; however it changed somewhat between the 5th and 8th sessions (e.g., self-confidence, academic/professional adaptation). In terms of dropouts from therapy, we observed a total of 54%. These numbers were closer with those reported in prior studies, namely Weirzbicki and Pekarik (1999) that reported 46.86% withdrawals from therapy and Garfield (1994) that pointed out more than 65% of clients dropped from psychotherapy before the 10th session. Given that, an early termination of therapeutic process may prevent clients from reaching a desirable recovery, since according to literature, a minimum of 11 to 13 sessions are needed for clients to a complete recovery (Lambert, 1997). We also tried to analyse the effect of goal agreement in cases of withdrawal, since various studies stated this element as important ingredient for improving the global therapeutic outcome (Mackrill, 2010, 2011; Tryon & Winograd, 2011). Therefore, we found a mixed results pattern in regard to this issue. This apparent inconsistency reinforces the idea that psychotherapy outcomes are not solely dependent on goal agreement, but also on relational depth and the therapist’s capacity to embody core facilitative conditions, such as empathy, congruence, and unconditional acceptance (Soares et al., 2026).We observed that when clients and therapists agreed on specific goals for therapy such as interpersonal relationship and prevention of drug consumption in 3rd session, those clients tend to remain in therapy, predicting so, eventually, better outcomes. This result was consistent with prior studies (Mackrill, 2010, 2011; Tryon & Winograd, 2011) that indicated goals consensus as an important element to foresee the quality of the therapeutic process. However, we did not observe the same pattern regarding self-confidence, emotional control and psychological wellbeing goals category. In these latter cases, on the contrary, the agreement on goals for therapy between therapists and clients were linked with cases of dropouts. These mixed results highlight what Defire and Hilsenroth (2011) mentioned about the fact that the relationship between goal consensus and therapeutic outcome after the 3rd session of therapy was not so clear. All these results raised more questions and hypotheses than answers. One possible hypothesis, for the fact that clients tend to continue the therapy when therapist had different goals for therapy, is that clients had not yet found satisfactory answers for their problems or needs, and they persisted. In others cases, when clients gave up therapy, even when they share common goals with therapists, may be due their perception of recovery and improvement or low levels of motivation and commitment in pursuing their goals. As referred by some authors, clients may end the treatment when perceived that they reach some satisfactory relieve, despite a clinical significant change or recovery have not been met yet (see Barrett et. al. 2008). This mixed pattern of results about goal consensus and its effects on dropouts from therapy, suggests a boarder influence of factors on dropouts. As literature refers, there are many variables such as motivation, involvement in therapy, self-efficacy perception, external constraints (e.g., financial issues) that intervene in outcome of therapeutic process (Bados, Balaguer & Saldanã; Barret et al, 2008). That´s why it´s very complex to understand the dynamic of dyads of therapists and clients, and therefore, the establishment of causal relationships concerning dropouts. Nevertheless, we cannot ignore the role of goal agreement in facilitating the establishment of therapeutic collaboration and therapeutic process itself. Because of that, it is important that therapy privilege the dialogue, identification and discussion of expectations and goals for doing therapy between therapists and clients. Also, a regular reformulation, monitoring of those goals throughout the course of therapy, and a constant feedback is essential (Barrett et al., 2008; Defire & Hilsenroth, 2011). With this study, we intend to implement a seed that rises the interest in studying more deeply the dynamic of dyads, between clients and therapists, and not only of clients or therapists entity alone, as it is more common to found in other national studies. Further work is needed, to understand about therapist-client goal agreement on therapy goals and its effect on therapeutic outcome, in particular, with a much larger sample. Dropouts on therapy need to be further understood, and the paths that guide to better therapy outcomes. In this sense, focusing exclusively on agreement metrics may overlook essential dimensions of the therapeutic process, as contemporary literature highlights the need to move “beyond technique” and consider psychotherapy as a dynamic, relational, and context-sensitive process (Oliveira et al., 2026). Ultimately, understanding the dynamics of therapist-client dyads requires a shift from a purely technical and outcome-oriented perspective toward a more relational, process-oriented, and co-constructive view of psychotherapy.
References
- Bados, A., Balaguer, G., & C., Saldaña (2007). The Efficacy of Cognitive-Behavioral Therapy and the Problem of Drop-Out. Journal of Clinical Psychology, 63, 585- 592.
View at Publisher | View at Google Scholar - Baldwin, S., Wampold, B., & Imel, Z. (2007). Untangling the Alliance–Outcome Correlation: Exploring the Relative Importance of Therapist and Patient Variability in the Alliance, Journal of Consulting and Clinical Psychology, 75 (6), 842–852. doi: 10.1037/0022-006X.75.6.842
View at Publisher | View at Google Scholar - Barrett, M., Chua, W., Crist-Christoph, P., Gibbons, M., Casiano, D., et al. (2008). Early withdrawal from mental health treatment: implications for psychotherapy practice. Psychotherapy, 45(2), 247-267.
View at Publisher | View at Google Scholar - Bordin, E.S. (1979). The generalizability of the psychoanalytic concept of the working alliance. Psychotherapy: Theory, Research, and Practice, 16, 252–260.
View at Publisher | View at Google Scholar - Cooper, M., & McLeod, J. (2007). A pluralistic framework for counselling and psychotherapy: Implications for research. Counselling and Psychotherapy Research, 7, 135-143.
View at Publisher | View at Google Scholar - Defire, J., & Hilsenroth, M. (2011). Starting off the right foot: Common factor elements in early Pyschotherapy process. Journal of Psychotherapy Integration, 21(2), 172-191.
View at Publisher | View at Google Scholar - Garfield, S.L (1994). Research on client variables in psychotherapy. In A.E. Bergin & S.L. Garfield (Eds.), Handbook of psychotherapy and behavior change (pp.821-830). New York: Wiley.
View at Publisher | View at Google Scholar - Horvath, A.O., & Bedi, R.P. (2002). The alliance. In J.C. Norcross (Ed.), Psychotherapy relationships that work: Therapist contributions and responsiveness to patients (pp. 37-69). New York: Oxford University Press.
View at Publisher | View at Google Scholar - Lambert, M. J (2004). Presidential address: What we have learned from a decade of research aimed at improving psychotherapy outcome in routine care. Psychotherapy Research, 17, 1–14.
View at Publisher | View at Google Scholar - Luborsky, L. (2000). A pattern-setting therapeutic alliance study revised. Psychotherapy Research, 1, 17–29.
View at Publisher | View at Google Scholar - Mackrill, T. (2011). Differentiating life goals and therapeutic goals: expanding our understanding of the working alliance. British Journal of Guidance & Counselling, 39 (1), 25-39.
View at Publisher | View at Google Scholar - Mackrill, T. (2010). Goal Consensus and Collaboration in Psychotherapy: An existential Rationale. Journal of Humanistic Psychology, 50(1), 96-107.
View at Publisher | View at Google Scholar - Mahoney, M. & Granvold, D. (2005). Constructivism and psychotherapy. World Psychiatry, 4 (2), 74-77.
View at Publisher | View at Google Scholar - Martin, D. J., Garske, J. P., & Davis, M. K. (2000). Relation of the therapeutic alliance with outcome and other variables: A meta-analytic review. Journal of Consulting and Clinical Psychology, 68, 438–450.
View at Publisher | View at Google Scholar - Norcross, J. C. (2002). Psychotherapy relationships that work: Therapist contributions and responsiveness to patients. New York: Oxford University Press.
View at Publisher | View at Google Scholar - Oliveira, F., Lucas, C. V., & Soares, L. (2026). Beyond technique: Conceptual advances in clinical surgery research. Journal of Clinical Surgery and Research, 7(1).
View at Publisher | View at Google Scholar - Santos, P., & Soares, L. (2024). Narrative therapy and constructivist perspective: An integrative review of complicated grief and effective therapeutic contributions. Psychology and Behavioral Science International Journal, 22(2), 556082.
View at Publisher | View at Google Scholar - Schinka, J., Velicer, A., & Wayne, F. (2003). Handbook of research: Research methods in Psychology (Vols. 2). New Jersey: John Wiley & Sons, Inc.
View at Publisher | View at Google Scholar - Schnur, J., & Montgomery, G. (2010). A Systematic Review of Therapeutic Alliance, Group Cohesion, Empathy, and Goal Consensus/Collaboration in Psychotherapeutic Interventions in Cancer: Uncommon Factors?. Clin Psychol Rev., 30(2), 238–247.
View at Publisher | View at Google Scholar - Soares, L. & Lemos, M. (2003). Questionário objetivos para a terapia. Unpublished document. Universidade do Porto.
View at Publisher | View at Google Scholar - Soares, L., Botella, L., Corbella, S., de Lemos, M. S., & Fernández, M. (2013). Diferentes estilos de clientes y construcción de la alianza con un terapeuta. Revista Argentina de Clínica Psicológica, 22(1), 27–36.
View at Publisher | View at Google Scholar - Soares, L., Zlochová, N., & Vyskcilova, M. (2026). Let’s remember the beautiful concepts Carl Rogers left us in clinical psychology: Unconditional positive regard, genuineness and empathic understanding. Open Access Journal of Addiction & Psychology, 8(3).
View at Publisher | View at Google Scholar - Swift, J., & Callahan, J. (2009). Early Psychotherapy Processes: An examination of client and trainee clinical perspective convergence. Clinical Psychological and Psychotherapy, 16, 228-236.
View at Publisher | View at Google Scholar - Steering Committee (2002). Empirically supported therapy relationships: Conclusions and recommendations of the Division 29 Task Force. In J. C. Norcross (Ed.), Psychotherapy relationships that work: Therapist contributions and responsiveness to patients (pp. 441-443). New York: Oxford University Press.
View at Publisher | View at Google Scholar - Tryon, G. & Winograd, G. (2011). Goal Consensus and Collaboration. Psychotherapy, 48 (1), 50–57.
View at Publisher | View at Google Scholar - Weirzbicki, M., & Pekarik, G. (1993). A meta-analysis of psychotherapy dropout. Professional Psychology: Research and Practice, 24, 190–195.
View at Publisher | View at Google Scholar
