

Research Article | DOI: https://doi.org/10.31579/ 2835-8147/047
Challenges & possible solution to hemodialysis use in Myanmar: preparedness beyond COVID-19 infections
- Khin Phyu Pyar 1*
- Moe Zaw Myint 2
- Win Kyaw Shwe 4
- Kyaw Thu Yein Lwin 3
- Lay Maung Maung 3
- Ye Min Hein 3
- Aung Zaw Htet 3
- Moe Htun Zaw 3
- Sai Aik Hla 2
- Ye Htook Maung 4
- Myo Maung Maung 4
- Min Aung Hein 3
- Zin Zin Aung 4
- Aung Kyaw Khine 5
- San Lin 6
- Kyaw Zaw Lin 5
- Tun Tun Oo 5
- Myat Kyaw 5
- Nyein Chan Ko 5
- Myat Ko Ko 5
- Thet Aung 4
1 Professor and Head/ Senior Consultant Physician and Nephrologist, Department of Medicine/Nephrology, Defence Services Medical Academy/ No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
2 Senior Consultant Physician, No. (2) Defence Services General Hospital (1000-Bedded), Nay Pyi Taw, Myanmar.
3 Consultant Nephrologist, Department of Nephrology, No. (1) Defence Services General Hospital (1000-Bedded), Yangon, Myanmar.
4 Consultant Nephrologist, Department of Nephrology, No. (2) Defence Services General Hospital (1000-Bedded), Nay Pyi Taw, Myanmar.
6 Consultant Nephrologist, Department of Nephrology, No. (1) Military Hospital (700-Bedded), Pyin Oo Lwin, Myanmar.
7 Consultant Nephrologist, Department of Nephrology, No. (2) Military Hospital (700-Bedded), Aung Ban, Myanmar.
8 Nephrology Fellow, Defence Services Medical Academy, Yangon, Myanmar.
*Corresponding Author: Khin Phyu Pyar, Research and Training Center ‘Physical and Chemical Materials Science’ Under Kyiv Taras Shevchenko University and NAS of Ukraine, Kiev, Ukraine.
Citation: Khin P. Pyar, Moe Z. Myint, Win K. Shwe, Yein Lwin KT, Lay M. Maung et al, (2024), Challenges & possible solution to hemodialysis use in Myanmar: preparedness beyond COVID-19 infections, Clinics in Nursing, 3(1) DOI:10.31579/ 2835-8147/047
Copyright: © 2024, Khin Phyu Pyar. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 January 2024 | Accepted: 17 January 2024 | Published: 23 January 2024
Keywords: end stage renal diseases (ESRD); renal replacement therapy; Home based dialysis therapy (HBDT); CAPD (continuous ambulatory peritoneal dialysis); hemodialysis (HD); COVID-19 infections
Abstract
Background: The number of patients with end stage renal diseases requiring renal replacement therapy has been increasing worldwide; they are managed with renal transplant, hemodialysis (HD), CAPD (continuous ambulatory peritoneal dialysis) or conservative treatment. In Myanmar, in center HD is the main form of renal replacement therapy. This study aimed to explore the challenges following COVID-19 infections among patients on maintenance hemodialysis (MHD) and to find possible solution for them. Methods: A cross-sectional descriptive study was conducted in 2023 among patients on MHD at selected public hospitals in Myanmar. Data were collected by using standardized forms and analysis was done. Results: This study involved 158 patients made up of 74 (46.8%) males and 84 (53.2%) females with a mean age of 50.52 ± 12.41 years. Duration of HD ranged from 3 months to 168 months. Most of the patients, 61.4% (97/158), were doing HD free of charge; one fourth (40/158) had to share cost for tubing and dialyzer (10 USD per session). The travelling time was as follows: less than 30 minutes in 40% (63/158); 31 to 60 minutes in 34% (53/158); 61 to 90 minutes in 7.6% (12/158); 91 to 120 minutes in 7% (11/158); 121 to 150 minutes in 7.6% (12/158); 151 to 180 minutes in 3.8% (6/158); and, more than180 minutes in 0.6% (1/158). They had good satisfaction to their health care personnel. Two third of them were anxious about infectious diseases like COVID-19 infection and less than 5% had mild depression. They did not have problem with administrative challenges such as ‘hospital discipline’. Concerning information on their experience with COVID-19 infection among HD colleagues over past 3 years was sad. Two third of them received booster dose to COVID-19 vaccination. They want dialysis at home during epidemic as they were afraid of being infectious. Either new HD centers or home-based dialysis therapy (HBDT) is required for those with travelling time 2 hours and above. Priority to COVID-19 vaccination should be given to those on maintenance HD particularly booster doses. Psychosocial support is necessary. Conclusions: Most of them received HD free of charge in public hospital; however, one quarter had to share cost for tubing and dialyzer. Nearly two third of patients had acceptable travelling time for an hour. New HD centers or HBDT is recommended for those having more than an hour travelling time. Booster vaccination for COVID-19 infections to those on MHD should be carried on. Psychosocial support program should be enhanced in addition to psychotherapy. Training program and preparation for HBDT should be launched. |
Introduction
CKD is a global problem that causes significant burden not only to the healthcare system but also to patients and their family. The number of people with CKD in the world is increasing; about 10 % of people suffer from CKD and 5 % of them need RRT (Fasipe OJ et al, 2019).
The number of people who were on kidney replacement therapy exceeded 3 million in 2017 and is projected to grow to 5·4 million by 2030. ESRD is causing challenges for both patient and their family as well as the government (Ivanov, D. et al, 2022) [12]. They are managed with renal transplant, hemodialysis (HD), CAPD (continuous ambulatory peritoneal dialysis) or conservative treatment. The population of Myanmar is 55 million and the number of chronic kidney disease is expected to be 5 million; the number requiring RRT would be 2.5 million. As living donor renal transplant is limited in Myanmar; renal replacement therapy either HD or CAPD can contribute to numerous clinical benefits. RRT as maintenance hemodialysis has been initiated in Myanmar since 1970 in Government hospital with one machine. Later, the number of Hemodialysis Centers (HDC) increased gradually; it was launched in private sector in 1996. At present, at least one HDC in each State or Division; Myanmar has 14 State and Divisions. The number of HD centers increased dramatically to nearly 200 centers over 20 years; however, they were situated mainly in major cities. Nearly 98% of cases were doing in-center HD in Myanmar [16]. Peritoneal dialysis (PD) was first use in Myanmar in 1970 particularly for acute kidney injury; later, CAPD was introduced. However, the number of patients on CAPD was less than one hundred; half in Yangon and half in remote areas. The cost of one session of HD (in-center) was 30-35 USD; it rose to 40-45 USD if transport charges were included. In Myanmar, the number of patients on HHD was less than ten; on the other hand, the number on continuous ambulatory peritoneal dialysis (CAPD) was less than 100 in the whole country. Being developing country, it was not easy to get in-center HD even with recommended dose- 3 time per week. Moreover, the cost of injection erythropoietin was 10 USD per dose [16]. COVID-19 infection had profound effect on patients with dialysis [3,4]; high prevalence, increased severity of infection one infected and high mortality rate were reported [1,5,6, 8,10]. COVID-19 vaccination (booster dose) has been given to patients on MHD [19]. This study aimed to explore the challenges following COVID-19 infections among patients on maintenance hemodialysis (MHD) and to find possible solution for future disaster/epidemics.
Methods
Study design and population
A cross-sectional descriptive study was conducted in 2023 in 3 selected public Hemodialysis Centers (HDC): Yangon (lower part of Myanmar), Nay Pyi Taw (central part of Myanmar), and Aung Ban (Eastern part of Myanmar). Data were collected by using standardized forms and analysis was done.
Operational definitions
Maintenance hemodialysis (MHD) was defined as hemodialysis done either twice a week or three times a week for more than two months in patients with end stage renal disease. Duration of maintenance hemodialysis was defined as total duration since first HD. End stage renal disease was defined as patients with chronic kidney disease stage 5.
Travel time to HD center was defined as the duration of total travel time from the patient’s residence to HDC which included the waiting time for public transport.
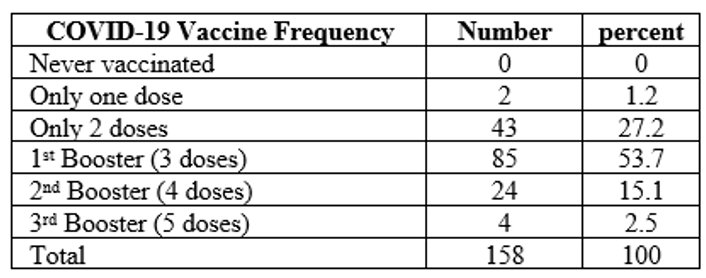
First booster dose vaccination was defined if the patient received total 3 dose of COVID-19 vaccine either same or different one. Second booster dose vaccination was defined if the patient received total 4 dose of COVID-19 vaccine either same or different one. Third booster dose vaccination was defined if the patient received total 5 doses of COVID-19 vaccine either same or different one.
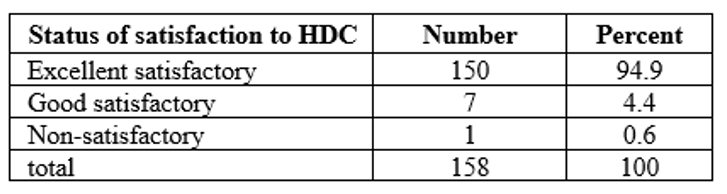
Satisfaction to attending HDC was categorized into excellent satisfactory, good/satisfactory, and non-satisfactory. Excellent satisfactory status was defined if the patient was extremely satisfied with treatment at HDC. Good satisfactory status was defined if the patient was satisfied with treatment at HDC. Non-satisfactory status was defined if the patient was not satisfied with treatment at HDC. They were recorded anonymously with separate voting paper.
Data collection and procedure
A cross-sectional hospital based descriptive study was conducted among patients doing in-center dialysis at government hospital; they were interviewed by physicians and nephrologists using structured questions in 2023. The timing of interview was end of HD session. The questions were based on key 5 elements. First was related with baseline characteristics (sex, age, height, duration of MHD); second was concerning with economic challenges (travel time, cost of HD, travel cost, cost of injection erythropoietin); third was psychosocial challenges like degree of satisfaction to their health care personnel and anxiety about infectious diseases like COVID-19 infection; fourth was administrative challenges such as ‘hospital discipline’, standard procedure for infection control and ‘COVID-19 prevention & treatment protocol’; fifth was information on their experience with COVID-19 infection among HD colleagues over past 3 years (number of infected cases, number of severe cases requiring hospital stay & number of dead cases); sixth was facts on COVID-19 vaccination (name of vaccine, number of doses, date of each vaccination); seventh was their preference on type of dialysis during epidemic and the reasons. The data were checked by two medical officers and then, supervision, completeness, and consistency of collected data were performed by the principle investigator. Data were collected by using standardized forms and analysis was done.
Statistical analysis
The collected data were entered into Microsoft Excel 2016 and exported to IBM SPSS Statistics for Windows, Version 23.0 (Armonk, NY: IBM Corp) for analysis. Descriptive statistics were presented as frequency and percentage for categorical variables and mean (standard deviation, SD) for continuous variables.
Results
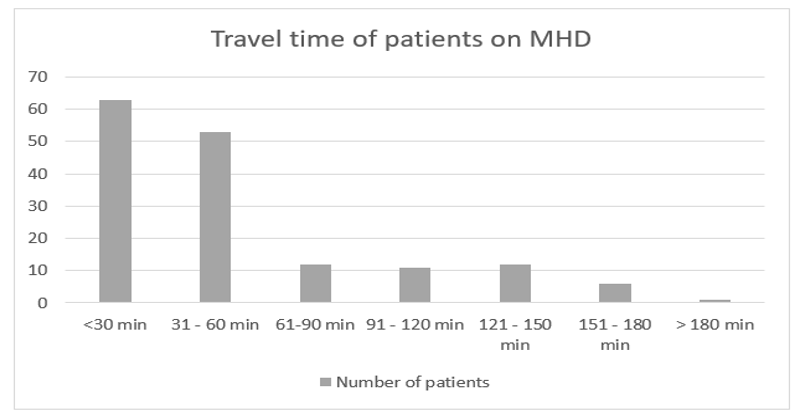
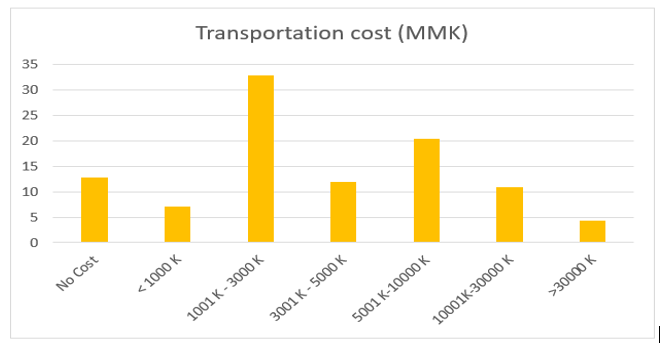
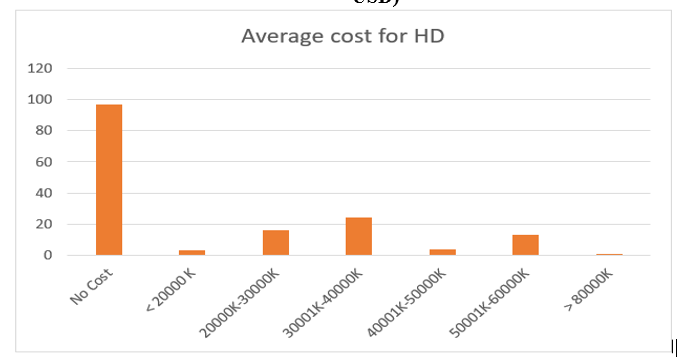
A cross-sectional descriptive study was conducted among patients on MHD at selected public hospitals in Myanmar. This study involved 158 patients made up of 74 (46.8%) males and 84 (53.2%) females. The mean age was 50.52 ± 12.41 years. Duration of HD ranged from 3 months to 168 months. Economic challenges included travel time, cost of HD, travel cost, and cost of injection erythropoietin. Figure (1) shows various travelling time of patients; less than 30 minutes in 40% (63/158); 31 to 60 minutes in 34% (53/158); 61 to 90 minutes in 7.6% (12/158); 91 to 120 minutes in 7% (11/158); 121 to 150 minutes in 7.6% (12/158); 151 to 180 minutes in 3.8% (6/158); and, more than180 minutes in 0.6% (1/158). In this study, the median travel time to HD center was 45 minutes (IQR 26- 120 minutes). The minimum travel time was 15 minutes; the maximum was 3 hours (180 minutes). Figure (3) illustrates the cost of each session of HD. Most of the patients, 61.4% (97/158), were doing HD free of charge; however, 25% (40/158) had to share cost for tubing and dialyzer (10 USD per session). The expense for transportation varied from 1USD to 10 USD per one session. Most of the patients 61.4% (97/158) received free of charge for HD; however, 25% (40/158) had to share cost for tubing and dialyzer (10 USD/session), less than one third of cost in private hospital. It is demonstrated in figure (2). The cost of injection erythropoietin was 10 USD per vial. Regarding psychosocial challenges like degree of satisfaction to health care personnel and anxiety about infectious diseases like COVID-19 infection, all patients were satisfied with service from health care workers concerned. Table (1) reveals satisfactory score to health care workers. Seventy-five percent of them were anxious about infectious diseases like COVID-19 infection; however, they believed that their protective efficacy with booster vaccination was good. In response to administrative challenges such as ‘hospital discipline’, standard procedure for infection control and ‘COVID-19 prevention & treatment protocol’, they compiled with hospital infection control rules and administrative protocol particularly related with COVID-19 infections.
Feelings on their colleagues with COVID-19 infection over 3 years (number of infected cases & number of dead cases) and their feelings were heart breaking. Before introduction of COVID-19 vaccine, in second wave, nearly one fourth of patients on MHD attending Yangon public HD center were infected. After first dose of vaccine, in third wave, Delta, half of patients were infected. Mortality rate was more than 33% in second wave and it dropped to 10% in third wave. Following completed vaccination and booster vaccination, the mortality rate dropped dramatically to 1-3% in fourth and fifth waves. Therefore, two third of patients in Yangon HD center was afraid of acquiring COVID-19 infection as they faced high infectivity and mortality among their colleagues in one HD center in second (the wild type and Alpha) and third wave (the Delta wave) of COVID-19 infections. They scared to come to HD center for HD during epidemics because of high risk of acquiring COVID-19 infection. They were worried about their selves regarding complications/severe infection and death. They felt sorry for those having severe infection and non-survivors. Their grief period lasted several months. Two third of them had anxiety and less than 5% had mild depression particularly after Delta wave of COVID-19 infection. Table (2) shows vaccination status; two third of them had booster dose. Their preference on type of dialysis during epidemic was home-based dialysis therapy (HBDT) in order to get non-infected.
Discussion
This study involved 158 patients with the mean age of 50.52 ± 12.41 years; their duration of HD ranged from 3 months to 168 months. The patients were facing economic challenges (travel time, cost of HD, travel cost, cost of injection erythropoietin). The minimum travel time was 15 minutes; the maximum was 3 hours (180 minutes). Those with longer travel time were from hilly region; Shan State. The expense for transportation varied from 1USD to 10 USD per one session. Most of the patients received free of charge for HD. However, 25% had to share cost for tubing and dialyzer (10 USD/session), less than one third of cost in private hospital. The cost of one session of HD (in-center) in private center was 30-35 USD; it rose to 40-45 USD if transport charges were included [17].
According to the study on cost per hemodialysis session in ASEAN countries was 25–70 US dollar and expensive if it is compared with average monthly income of every country [7]. The inflation caused the changes in cost of HD, its accessories and drugs. Either new HD centers or home-based dialysis therapy (HBDT) is required for those with travelling time 2 hours and above. CAPD (continuous ambulatory peritoneal dialysis) would be better than home hemodialysis (HHD) in resource poor setting [18]. The burden of dialysis was faced by both developed and developing countries. The study from Australia identified the importance of financial hardships though HDC were supported by government [21]. The report from Indonesia mentioned that hemodialysis adherence was directly affected by higher family income, distance < 20> Even France and UK highlighted the importance of travel time to HDC [20, 24]. The researchers from Australia found that geographical barriers were important in long term adherence [21]. Haemodialysis requires infrastructures and facilities such as electricity, intense water consumption and buildings; it seems to have upstaged peritoneal dialysis both in demand and supply (Ivanov, D. et al; 2022). Half of the patients in this study required an hour travel time to HDC. There are 14 States and Divisions in Myanmar. Seven States occupy hilly regions where they are less populated; they are Shan State, Kachin State, Chin State, Rakhine State, Kayah State, Kayin State and Mon State. Seven Divisions are non-hilly areas; thus, they are densely populated. They are Yangon Division, Naypyitaw Division, Mandalay Division, Sagaing Division, Bago Division, Magway Division and Irrawaddy Division. Current total population in Myanmar is 55.39 million (Myanmar Population Clock); and, it is 53.4 million in 2017. The findings from United Kingdom pointed out that the adherence to treatment, hemodialysis, was inversely proportionate with travel time; they also recommended to build a new HDC if travel time was more than 45 minutes. Therefore, we need more HDC and human resources. Reallocation of man, materials and money to kidney health by modification of health policy should be done as suggested by other study [2]. Cost of HD was shared in one fourth of patients in this study. Travel cost was not cheap; erythropoietin too. Expense for transportation should be handled in collaboration with transport ministry and ministry of health. We need economic support for them; charity job would help to some extent. The role of health policies was the main key player in achieving equity in dialysis care and outcomes. Dialysis burden was a global challenge even in rich countries [15]. If possible, home based dialysis therapy (HBDT) should be launched in Myanmar; CAPD would be good option as HBDT. Report from one analysis revealed that most developed countries provided CAPD at a lesser expense to the healthcare system than HD; however, PD was the same cost in developing countries [11]. It is better to make shared decision with the patient for choosing in-center HD or HBDT. However, the study from Switzerland showed that the majority of patients preferred in-centre haemodialysis. Concerning challenges like degree of satisfaction to their health care personnel all patients were satisfied with service from health care workers concerned; they compiled with hospital infection control rules and administrative protocol particularly related with COVID-19 infections. They were worried about their selves regarding complications/severe COVID-19 infection and death. Two third of them had anxiety about infectious diseases like COVID-19 infection; it was related with their experience in COVID-19 epidemic. The information on their experience with COVID-19 infection among HD colleagues over past 3 years (number of infected cases, number of severe cases requiring hospital stay & number of dead cases) was very poor. Before vaccination, in second wave, nearly one fourth of patients on MHD in Yangon public center were infected. After first dose of vaccine, in third wave, Delta infection, half of patients were infected. Mortality rate was more than 33% in second wave and 10% in third wave. Following completed vaccination and booster vaccination, the mortality rate dropped dramatically to 1-3%. Concerning the reaction to COVID-19 infection over 3 years, one third of them was afraid of acquiring COVID-19 infection as they face high infectivity and mortality among their colleagues in one HD center in second (the wild type and Alpha) and third wave (the Delta wave) of COVID-19 infections. Priority of vaccination should be given to those on maintenance HD particularly booster doses. They scared to come to HD center for HD because of high risk of acquiring COVID-19 infection. They were worried about their selves regarding complications/severe infection and death. They felt sorry for those having severe infection and non-survivors. Their grief period lasted several months. Two third of them had anxiety and depression particularly after Delta wave of COVID-19 infection. The researcher from Middle East found that patients under hemodialysis treatment suffered from depression, anxiety, and poor quality of life [23]. Psychosocial challenges should be managed in collaboration with psychiatrist. One qualitative research done in 2018 pointed out the need for social support and concern, empathy, companionship in everyday needs, social support and concern, and good-quality dialysis [22]. Even without COVID-19 pandemic, their physical quality of life became worse as dialysis vintage lengthened; their mental quality of life declined over time within a relatively short period among older maintenance hemodialysis patients [19]; psychosocial distress was emphasized in other study too [14]. Therefore, psychosocial support is essential for them. Reaction to administrative challenges such as ‘hospital discipline’, standard procedure for infection control and ‘COVID-19 prevention & treatment protocol’ was good; they compiled with hospital infection control rules and administrative protocol particularly related with COVID-19 infections. The fact on COVID-19 vaccination (name of vaccine, number of doses, date of each vaccination) was excellent. In view of vaccination status to COVID-19,99% were vaccinated. They were in the priority list for booster regimen in view of poor immunity. They were lucky as two third of them had booster doses. In order to get non-infected, their preference on type of dialysis during epidemic was home-based dialysis therapy (HBDT). They barely know CAPD (continuous ambulatory peritoneal dialysis) or home hemodialysis (HHD). Therefore, training for HBDT is highly recommended for both patients on MHD and health care workers. Their preference on type of dialysis during epidemic was HBDT in order to get non-infected. They barely know CAPD or HHD. Therefore, not only the training for CAPD/HHD but also the essential materials should be prepared for future.
Limitation of study
There are several limitations in this study. The sample size was small as it was conducted only in three Government HD centers. The analysis would be better if larger number of patients and number of HDC were included. Moreover, only government funded centers were included in the study as the patients from private HDC were reluctant to give informed consent. The socioeconomic status of patients in this study may be different from that of private center; different form of challenges. Though the travelling distance was constant, the travel time was variable. The waiting time for public transport (bus) varied from 20 to 30 minutes unlike the transport system in developed countries. Moreover, inflation status determined the cost of consumables like dialyzer, tubing, erythropoietin injection and dialysates.
Conclusion
Three fourth of them received HD free of charge in public hospitals; however, one fourth of them had to share cost for tubing and dialyzer. Nearly two third of patients had acceptable travelling time for an hour. New HD centers or HBDT were required for one third of cases having more than an hour travelling time. Counselling and psychological support are recommended for those having psycho-social stress particularly after COVID-19. Resource allocation to renal replacement therapy should be encouraged at ministry level. COVID-19 vaccination not only reduced prevalence of acquiring COVID-19 infection and severity of infection but also decreased mortality in patients on MHD. Moreover, it enhanced their confidence. Implementation of booster vaccination for COVID-19 infections to those on MHD should be done in addition to keeping social distance, maintaining personal hygiene, quarantine, and isolation. Both the training for CAPD/HHD and preparation for the essential materials should be done for future infectious diseases.
Recommendations
To improve accessibility to HD center, new HDC is required if travel time is more than 60 minutes. On the other hand, HBDT with reasonable price should be second option. As CAPD is relatively cheaper than HHD, expansion of CAPD program should be done at ministry level. Transport and communication services should be promoted. Sustainability of dialysis fluids, tubing and dialyzer should be maintained. COVID-19 booster vaccination should be maintained. To promote affordability, dialyzers and dialysis solutions should be produced locally to cut down the costs of hemodialysis and CAPD. Economic support and charity program should be encouraged.
Acknowledgment
We are thankful to Professor Ko Ko Lwin, Professor Kyaw Zay Ya, Directorate of Medical Services; Professor Myint Zaw (Yangon HDC), Professor Aung Myat Kyaw (NayPyi Taw HDC), Professor Myo Thant (Pyin Oo Lwin HDC) & Professor Saw Yan Naing (Aung Ban HDC) for their administrative support. We are also grateful to all patients and health care personnel included in this study.
Ethical consideration
The data collection using standardized case report forms was approved by Hospital Ethics Review Committee of Defence Services General Hospital, Mingaladon. Informed consent was taken from both patients and their attending nephrologists and physicians. Privacy and
confidentiality of information was maintained throughout the study process.
Conflict of interest
There was no COI.
Funding
No funding was obtained.
References
- Chu D.-T., Vu Ngoc S.-M., Vu Thi H., Nguyen Thi Y.-V., Ho T.-T., et. al., (2022). COVID-19 in Southeast Asia: Current status and perspectives. Bioengineered, 13(2), 3797–3809.
View at Publisher | View at Google Scholar - Crews, D. C., & Novick, T. K. (2020). Achieving equity in dialysis care and outcomes: The role of policies. Seminars in Dialysis, 33(1), 43–51.
View at Publisher | View at Google Scholar - Demiray, A., Kanbay, A., & Kanbay, M. (2022). Long-term effect of COVID-19 infection on hemodialysis patients: Should we follow hemodialysis patients more closely? Clinical Kidney Journal, 15(3), 369–371.
View at Publisher | View at Google Scholar - El Karoui, K., & De Vriese, A. S. (2022). COVID-19 in dialysis: Clinical impact, immune response, prevention, and treatment. Kidney International, 101(5), 883–894.
View at Publisher | View at Google Scholar - Fisher, M., Yunes, M., Mokrzycki, M. H., Golestaneh, L., Alahiri, E., et. al., (2020a). Chronic Hemodialysis Patients Hospitalized with COVID-19: Short-term Outcomes in the Bronx, New York. Kidney360, 1(8).
View at Publisher | View at Google Scholar - Fisher, M., Yunes, M., Mokrzycki, M. H., Golestaneh, L., Alahiri, E., et. al., (2020b). Chronic Hemodialysis Patients Hospitalized with COVID-19: Short-term Outcomes in the Bronx, New York. Kidney360, 1(8).
View at Publisher | View at Google Scholar - Hyodo, T., Yamashita, A. C., Hirawa, N., Isaka, Y., Nakamoto, H., et. al., (2022). Present status of renal replacement therapy in lower-middle-income Asian countries: Cambodia, Myanmar, Laos, Vietnam, Mongolia, and Bhutan as of June 2019 (before COVID-19), from the interviews of leading doctors in every country: (Duplicated English publication from “the special Japanese edition of educational lectures in the 64th annual meeting of the Japanese Society for Dialysis Therapy”). Renal Replacement Therapy, 8(1), 54.
View at Publisher | View at Google Scholar - Ibernon, M., Bueno, I., Rodríguez-Farré, N., Ruiz, P., Sánchez, A., et. al., (2021). The impact of COVID-19 in hemodialysis patients: Experience in a hospital dialysis unit. Hemodialysis International, 25(2), 205–213.
View at Publisher | View at Google Scholar - Ishiwatari A., Yamamoto S., Fukuma S., Hasegawa T., Wakai, S., et. al., (2020). Changes in Quality of Life in Older Hemodialysis Patients: A Cohort Study on Dialysis Outcomes and Practice Patterns. American Journal of Nephrology, 51(8), 650–658.
View at Publisher | View at Google Scholar - Jin G., Ding Z., Li G., Hu J., Liu J., et. al., (2021). Clinical course of patients on maintenance hemodialysis and COVID-19: A retrospective longitudinal study. International Journal of Medical Sciences, 18(11), 2366–2371.
View at Publisher | View at Google Scholar - Karopadi A. N., Mason G., Rettore E., & Ronco, C. (2013). Cost of peritoneal dialysis and haemodialysis across the world. Nephrology Dialysis Transplantation, 28(10), 2553–2569.
View at Publisher | View at Google Scholar - Kovesdy C. P. (2022). Epidemiology of chronic kidney disease: An update 2022. Kidney International Supplements, 12(1), 7–11.
View at Publisher | View at Google Scholar - Kukuh Ardian, Endang Sutisna Sulaeman, & Arief Suryono. (2017). Social Economic Equity in the Utilization of Hemodialysis Among Patients with Chronic Renal Failure Under National Health Insurance Plan at Dr. Moewardi Hospital, Surakarta. Journal of Health Policy and Management, 2(1), 28–41.
View at Publisher | View at Google Scholar - Lee J., Steel J., Roumelioti M.-E., Erickson S., Myaskovsky L., et. al., (2020). Psychosocial Impact of COVID-19 Pandemic on Patients with End-Stage Kidney Disease on Hemodialysis. Kidney360, 1(12).
View at Publisher | View at Google Scholar - Li. P. K.-T., Chan. G. C.-K., Chen, J., Chen, H.-C., Cheng, Y.-L., et. al., (2021). Tackling Dialysis Burden around the World: A Global Challenge. Kidney Diseases, 7(3), 167–175.
View at Publisher | View at Google Scholar - Pyar, K. P. (2022a). Initial presenting symptoms andseverity of SARS-CoV-2 Wild type, theDelta variant and the Omicron variant infected cases in early fourth wave ofepidemics in Myanmar. Research Review.
View at Publisher | View at Google Scholar - Pyar, K. P. (2022b). Equity of Maintenance Hemodialysis in Myanmar: Cross-Sectional Descriptive Study. Journal of Biomedical Research & Environmental Sciences, 3.
View at Publisher | View at Google Scholar - Pyar, K. P. (2022c). Equity of Maintenance Hemodialysis in Myanmar: Cross-Sectional Descriptive Study. Journal of Biomedical Research & Environmental Sciences, 3.
View at Publisher | View at Google Scholar - Pyar. K. P., Myint. M. Z., Hla. S. A., Hlaing. S. W., Aung. A., et. al., (2022). Effectiveness of 4 doses of COVID-19 vaccine in patients on maintenance hemodialysis in 5th wave of COVID-19 infection in Myanmar: Do we need 5 doses? International Journal Of Medical Science And Clinical Research Studies, 2(12), 1496–1503.
View at Publisher | View at Google Scholar - Richard J.-B., Aldigier J.-C., Le Mignot L., Glaudet F., Ben Said M., et. al., (2009). Equity of accessibility to dialysis facilities. Studies in Health Technology and Informatics, 150, 777–781.
View at Publisher | View at Google Scholar - Scholes-Robertson N. J., Gutman T., Howell M., Craig J., Chalmers R., et. al., (2022). Clinicians’ perspectives on equity of access to dialysis and kidney transplantation for rural people in Australia: A semistructured interview study. BMJ Open, 12(2), e052315.
View at Publisher | View at Google Scholar - Shahgholian N., & Yousefi H. (2018). The lived experiences of patients undergoing hemodialysis with the concept of care: A phenomenological study. BMC Nephrology, 19(1), 338.
View at Publisher | View at Google Scholar - Um-e-Kalsoom Khan, S., & Ahmad I. (2020). Impact of hemodialysis on the wellbeing of chronic kidney diseases patients: A pre-post analysis. Middle East Current Psychiatry, 27(1), 54.
View at Publisher | View at Google Scholar - White P., James V., Ansell D., Lodhi V., & Donovan K. L. (2006). Equity of access to dialysis facilities in Wales. QJM: An International Journal of Medicine, 99(7), 445–452.
View at Publisher | View at Google Scholar
