

Research Article | DOI: https://doi.org/10.31579/2834-8486/014
BRANCHED CHAINED AMINO ACIDS ENRICHED BAR AND CHRONIC LIVER DISEASE: A CASE STUDY
- Khadija Arshad1
- Rabia Naz *
- Rabia Naz
- Rabia Naz
Department of Food Science and Human Nutrition, Kinnaird College for Women, Lahore Pakistan.
*Corresponding Author: Rabia Naz, Department of Food Science and Human Nutrition, Kinnaird College for Women, Lahore Pakistan.
Citation: Khadija Arshad , Rabia Naz , Mahnaz Nasir , Nadia Akram
(2023), BRANCHED CHAINED AMINO ACIDS ENRICHED BAR AND CHRONIC LIVER DISEASE: A CASE STUDY. Biomedical and Clinical Research, 2(6); DOI:10.31579/2834-8486/014
Copyright: © 2023, Ayesha Fazal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 November 2023 | Accepted: 17 November 2023 | Published: 29 November 2023
Keywords: Aromatic amino acids, branched chained amino acid, glutamine, Chronic liver disease, protein calorie malnutrition
Abstract
Nutritional intervention with branched-chain amino acid (BCAA) is reported to increase survival of patients with decompensate cirrhosis. Purposely, a branched chain amino acids rich snack was developed and its effect on serum albumin and total protein levels of chronic liver disease patient was assessed. Pumpkin seeds, lentils and brown sugar were used in the preparation of the product to fulfill the daily BCAA requirement of the patient. The evaluated product was considered acceptable for chronic liver disease patient with serum albumin levels below 4g/dL. A 6- week trial was conducted in which patient was served with a bar as an evening snack to determine its effectiveness in increasing the serum albumin levels. Significant increase in serum albumin levels were observed; raising the values from 3.82 g/dL to 4.9 g/dL and total protein levels from 7.04 g/dL to 8.14 g/dL. Thus, the study infers that there was an inverse association between BCAA enrich snack food and serum profile of the patient.
Introduction
Protein calorie malnutrition (PCM) is common in all stages of liver disease especially in patients with cirrhosis. Liver cirrhosis refers to the abnormal condition which exhibits the development of fibrosis and depletion of branched chained amino acids (BCAAs) to fulfill the energy demand of body. Liver disease can adversely affect the nutritional status as well as the amino acid metabolism of human body and it result in hepatic dysfunction and alteration in serum protein levels. Predominantly, liver fails to metabolize proteins and the ratio of branched chained to aromatic amino acids decreases and resulted in macro as well as micronutrient deficiencies (Buchman, 2006 and Holecek, 2013). Interventions of BCCA are recommended to CLD patients for their exceptional pharmacological characteristics, detoxification of ammonia to glutamine (GLN) and reduced concentrations in liver cirrhosis. Many studies have shown inhibitory effect of BCAAs on proteolysis. In the skeletal muscles, the amino group of BCAAs is transferred to alphaketoglutarate by aminotransferase. The catabolism of BCAAs depends on the mitochondrial oxidation of the Branched chained keto amines (BCKA). The BCAAs supplementation focuses on three main areas. First, thetreatment of hepatic encephalopathy; second is regeneration of hepatic tissue and the third is prevention and treatment of hepatic cachexia (Peng, 2007). Consumption of BCAAs rich sources like dairy and plant-based proteins can reduce hyperammonemia, increase serum albumin concentration and bring a positive nitrogen balance in liver patients (Marchesini, 2005). Among the plant-based sources, pumpkin seed and lentil contained 34.56 to 58.8% protein (Glewet al., 2006) and 19.5 to 49.3%, respectively (Nosworthy et al., 2017) with high level of BCAA (isoleucine, leucine and valine). Therefore, keeping in view the pathophysiology of CLD patients and their compromised nutritional status cost effective ingredients (pumpkin seed and lentil) rich in BCAAs were chosen to develop a meal replacement bar. Further, total protein and serum albumin levels in patient were evaluated after intervention of BCAA enriched bar.
Materials & Methods
Current study was based on quasiexperimental design with pre-testing and posttesting. A patient suffering from CLD was chosen as a subject for the study. The experimental snack bar enriched with BCAA was developed at Food Science Laboratory of Food Science and Human Nutrition Department, Kinnaird College for Women, Lahore. For the development of product economical and readily available ingredients were selected (pumpkin seeds, lentils and brown sugar) and procured from the local market. The reason of the selection of these ingredients was based on their high BCAAs content. Pumpkin seeds were roasted and finely ground into powder. Lentils were boiled, dried and grinded until a fine powder was achieved. Brown sugar syrup was prepared by adding half cup water to one cup brown sugar. All powdered ingredients were mixed with sugar syrup to mold into shape of a bar. The product was made using simple procedures so that it can be easily prepared when required. The prepared bars were stored in air tight container till the end of intervention period. At the end of study, total proteins and serum albumin content of the patient were analyzed.
Base line assessment/ Medical History
The patient was a 65 years old man with a body weight of 80 kg & 5’2-inch height and the medical history of esophageal varices and mild congestive gastropathy in body and antrum of stomach. The pylorus and fundus were found to be normal as revealed by endoscopy. Test case was recently diagnosed with positive hepatitis C virus with slight scarring in liver and had an early stage of developing liver cirrhosis. The medications included the drugs for chest infection and diastolic dysfunction. The radiology report of liver revealed its size (14 cm) and texture (coarse). No focal lesion was seen. There was no intra/extra hepatic biliary dilation. Gall bladder wall was normal, no mass and no stone was found. Duct was not dilated and no focal lesion of parenchyma was found. Spleen was of normal size (10cm). No mass or stone was found in either of the kidneys. Urinary bladder had normal wall thickening and no enlarged lymph nodes were found.
Nutritional Intervention
Serum albumin levels and total protein levels before and after the nutrition intervention were analyzed to investigate the effect of intervention. A patient with serum albumin level less than 4 g/dL and no history of antidiabetic drugs or intravenous albumin was selected for intervention. Best method for analyzing the effect of BCAAs supplementation is the Fisher’s method which measures the ratio of BCAAs and AAA. Method used in this study is the serum albumin level because it is inexpensive and simple. The study protocol was approved by the ethical committee of the hospital and informed consent was obtained from the subject. Liver cirrhosis was examined from documented laboratory data. The trial started on 9th January 2017 and ended on 13th February 2017 i.e. six weeks. First week was the trial period so that if the patient feels any side effects then withdraw the consumption of the BCAAs enriched bar. The caretaker was guided to keep the bars refrigerated and to give it to the patient as an evening snack. The patient was not recommended to stop eating any of the other protein sources. The medications were also continued as prescribed by the health care provider. The effect of the nutrition intervention was assessed after sixweek trial by the nutrition marker: serum albumin protein and total protein.
2.3. Biochemical Assessment Serum albumin level is a good indicator of protein nutritional status. Normal serum albumin levels are 3.5-5.5 g/dL while in liver cirrhosis, these levels decline to less than 3.5 g/dL. Total protein levels represent the total protein blood; this includes two major proteins i.e. albumin and globulin. Albumin in blood prevent albumin from leaking out of the vessels. Normal values for total protein are 60g/L to 83g/L. The serum albumin level and total proteins was estimated by following the protocol of standard laboratory techniques.
3. Results and Discussion
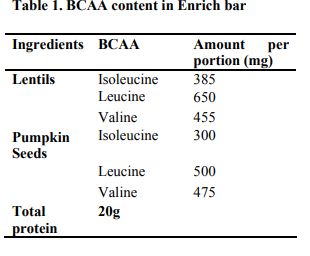
The BCAA in the enriched bar was estimated using the USDA Food Composition table and the results are presented in Table 1.The information is represented for 100 grams of the bar. Lentils and pumpkin seeds show high BCAA content as compared to other sources; isoleucine 385mg, leucine 650mg,445mg in lentils. The BCAA breakdown of pumpkin seeds was; isoleucine 300mg, leucine 500mg and valine 475 mg.
The outcomes of the present intervention study resulted in a significant increase in the total proteins and serum albumin as shown in Fig 1. Fig. 1 shows the pre and post-test serum albumin levels. Before the nutritional intervention, the serum albumin level was estimated as pre-test value. It was found out to be 3.82 g/dL. When the BCCAs rich bar was administered to the patient as an evening snack for 6 weeks trial, the effect of the bar was inferred. Liver function test was conducted and a prominent increase in serum albumin levels was found.
Fig. 1 shows pre and post-test of total protein levels of patient after the intervention period. Low levels are expected in early liver cirrhotic patients. Laboratory test revealed similar results. Prior to the administration of the bar total protein was found to be 7.04 g/dL. The trial lasted for 6 weeks and improved the total protein levels to 8.14g/dL.
Discussion
The study aimed to achieve interconnected outcomes. The focus was laid on the development of a BCCAs rich bar from natural and economical sources for patients with compromised liver status. This required the sensory evaluation tests from the trained panelists followed by the clinical trial which was aimed to last for 6 weeks. The results were compiled for the validation of the developed product. Also, the biochemical values obtained after the clinical trial were compiled and documented. A previous study records, protein malnourishment in liver patients. Since these attributes of the subject become the primary objective of clinical trial. Biochemical analysis was done as pretest on the subject; serum albumin levels were measured and after 6 weeks trial, it was post tested by another liver function test. A patient with early stage liver patient diagnosed with hepatitis C few months’ backs was selected for the clinical trial. The BCAAs enriched bar was given as an evening snack for 6 weeks by the caretaker of the patient. Similarly, Nakaya et al., 2007 done a randomized study on 48 patients with liver cirrhosis and hepatitis positive C for 3 months which consisted of two groups; one was given BCCAs rich snack and other group was given an ordinary snack. Each patient was given BCAAs enrich bar as a late evening snack. During the clinical trial each patient was instructed on the consumption of the bar. The biochemical parameters improved after the administration of the bar; serum albumin levels, nitrogen balance and quality of life improved. There was an evident increase in serum albumin levels in BCAAs group from mean values of 2.95 g/dLto 3.61 g/dL after 3 months. Mean Total protein levels improved from 6.9 g/dL to 7.3 g/dL. Unlike the snack group who were given ordinary snack at evening, no evident improvement was seen after 3 months trial in serum albumin and total protein values. Nishiguchi and Habu’s (2004) studied the early stage liver patients who were positive for HCV and had serum albumin levels below 4 g/dL. Half of them were given BCCAs supplement and half of them were assigned to the control group. Evaluation of the patients was done before the nutrition intervention was given and it was repeated after 2 years at 1 year interval. The patients were divided into three classes, class 1 included decompensated liver patient with serum albumin levels below 3.5 g/dl, class 2 consisted of compensated patients with serum albumin levels above 4 g/dL and class 3 included patients for control group.
Conclusion
Conclusively; patient with compensated stage revealed significant improvement in biochemical parameters because of intervention of BCCAs enriched bar. The above studies prove that BCCAs enriched bar is a good option for significantly improving serum albumin and total protein levels.
References
- Buchman, A. S.2006. Nutritional support in patients with chronic liver disease.Nature clinical practice gastroenterology and heptology, vol 2:202.
View at Publisher | View at Google Scholar - Nakaya, Y., Okita, K., Suuki, K., Moriwaki, H., Kato, A., Miwa, Y., &Shiraishi, K. 2007. BCAA-enriched snack improves state of cirrhosis. Nutrition, 23: 113- 120.
View at Publisher | View at Google Scholar - Muto, Y., Sato, S., Watanabe, A., &Moriwaki, H.2005. Effects of Oral Branched chained amino acid granules on eventfree survival in patients with liver cirrhosis. Clinical Gastroenterology and Hepatology,3, 705-713.
View at Publisher | View at Google Scholar - Henkel, A. S., & Buchman, A. L. 2006.Nutrition support in patients with chronic liver disease. Gastroenterology andHepatology,3(4): 202-209.
View at Publisher | View at Google Scholar - Giulio Marchesini, G. B. 2003. Nutritional supplementation with branched-chain amino acids in advanced cirrhosis: a double-blind, randomized trial. Gastroenterology , 1792–1801.
View at Publisher | View at Google Scholar - Glew, R. H., Glew, R. S., Chuang, L. T., Huang, Y. S., Millson, M., Constans, D., &Vanderjagt, D. J. (2006). Amino acid, mineral and fatty acid content of pumpkin seeds
View at Publisher | View at Google Scholar - Holecek, M. 2013. Branched-chain amino acids and ammonia metabolism in liver disease:. Nutrition , 1186–1191. Kazuto Tajiri, Y. S. 2013. Branched-chain amino acids in liver diseases. World Journal Gastroenterology , 7620– 7629.
View at Publisher | View at Google Scholar - Kelly Cheung, S. S. 2010. Prevalance and occurance of malnutrition in patients with advanced liver disease and nutrition management strageries. Clinical gastroentrology and heptology , 117-125.
View at Publisher | View at Google Scholar - Khan, T. S. 2014. Protein Calorie Malnutrition in Liver Cirrhosis. Nutrition and Food sciences . Plauth, M. M. 1997. ESPEN guidelines for nutrition in liver disease and. Clinical Nutrition , 43-55 .
View at Publisher | View at Google Scholar - Marchesini, G. 2005. Branched-Chain Amino Acid Supplementation in Patients with Liver. Journal of Nutrition , 1597- 1600.
View at Publisher | View at Google Scholar - Nosworthy, M. G., Tulbek, M. C., & House, J. D. (2017). Does the concentration, isolation, or deflavoring of pea, lentil, and faba bean protein alter protein quality?.Cereal Foods World, 62(4), 139-142.
View at Publisher | View at Google Scholar - Shuhei Nishiguchi, D. H. 2004. Effect of oral supplementation with branched-chain amino acid granules in the early stage of cirrhosis. Heptology research , 36- 41.
View at Publisher | View at Google Scholar - Sibbald, B. (1998). Understanding controlled trials: Why are randomised controlled trials important? BMJ ,316.
View at Publisher | View at Google Scholar - Silva, M. 2015. Nutrition in Chronic liver Disease. Portuguese journal of Gastroenterology , 268-279.
View at Publisher | View at Google Scholar - Starkie Sowers, C. 2009. A Primer On Branced Chained Amino Acids. Huntington College of Health Sciences.
View at Publisher | View at Google Scholar - Wassem Juakiem, M. D. (n.d.). Nutrition in Cirrhosis and chronic liver disease.
View at Publisher | View at Google Scholar - Yasutoshi Muto, 2005. Effects of Oral Branched-Chain Amino Acid Granules on Event-Free Survival in Patients With Liver Cirrhosis. Clinical Gastroenterology and Hepatology , 705-713.
View at Publisher | View at Google Scholar
