

case report | DOI: https://doi.org/10.31579/2834-796X/060
Atrial septostomy in a patient with severe pulmonary hypertension and hypoxia: A therapeutic conundrum
- Amit Mandal *
- Oommen George
Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
*Corresponding Author: Amit Mandal, Department of Cardiology, Christian Medical College, Vellore, Tamil Nadu, India.
Citation: Amit Mandal, Oommen George (2024), Atrial septostomy in a patient with severe pulmonary hypertension and hypoxia: A therapeutic conundrum, International Journal of Cardiovascular Medicine, 3(2); DOI:10.31579/2834-796X/060
Copyright: © 2024, Amit Mandal. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 March 2024 | Accepted: 18 March 2024 | Published: 03 April 2024
Keywords:
Abstract
Atrial septostomy may be considered in individuals with severe pulmonary arterial hypertension and right heart failure, despite maximal medical therapy, as a palliative procedure or bridge to transplant. Low oxygen saturation is a relative contraindication to atrial septostomy. Here, we present a young female patient with IPAH who received maximal target medication and was admitted to our hospital due to advanced right heart failure. She subsequently underwent successful atrial septostomy.
Background
Atrial septostomy (AS) is an additional strategy for the treatment of right ventricular failure (RVF) from severe pulmonary arterial hypertension (PAH). (1)
There are several reasons that justify its use:
a. the deleterious impact of RVF on patient survival (2)
b. the unpredictable response to medical treatment.
c. the disparity in the availability of these treatments throughout the world and
d. the limited access to lung transplantation.
Hence AS is currently recommended as palliative procedure or bridge to transplant for patients with severe PAH and intractable right heart failure despite maximal medical therapy, including optimized PAH specific agents and inotropes. (3)
Atrial septostomy is a right-to-left shunt that connects right and left atrial cavities. This atrial defect decompresses the RV and helps in delaying the catastrophic event of RV failure. Also, the defect shunts more blood to the left side thereby increases cardiac output, which, despite decreased oxygen concentration from right-to-left shunting, improves overall oxygen delivery to the peripheral tissues. Decompressing the right atrium sometimes dramatically improves signs and symptoms of systemic congestion like ascites and lower extremity edema. (4)
In this paper, we discussed a case 43-year-old lady with severe PAH with hypoxia who underwent successful atrial septostomy, discussing the role of atrial septostomy and the management dilemma in such patients.
Case Presentation
A 43-year-old woman with IPAH had received maximal target medications including oral phosphodiesterase type-5 inhibitor, endothelin receptor antagonist, and prostacyclin receptor agonist. Other than IPAH, she had no remarkable past medical history. In March 2024, she developed worsening right heart failure with peripheral edema, oliguria, and worsening of dyspnea. Upon admission, her systolic blood pressure was 108/72 mmHg, pulse rate was 110 beats/min, SPO2 was 92% in room air, and respiratory rate 20/min. Physical examinations revealed a elevated jugular venous pressure, a grade II pansystolic murmur, and a palpable heave at the left lower sternal border with loud P2. Laboratory data showed anemia with hemoglobin 710.4 g/dL, and elevated NT-pro BNP of 15459 pg/mL. Trans-thoracic echocardiogram revealed a marked dilated RA and right ventricle (RV), in addition to a small and compressed left atrium (LA) and left ventricle (LV) with severe TR (Figure 1).
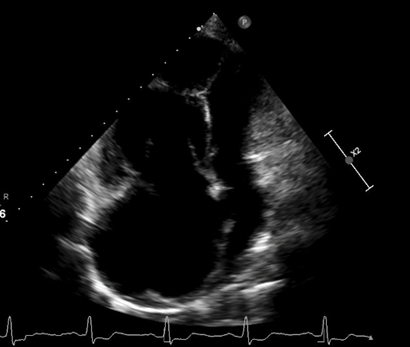
Figure 1: Trans-thoracic echocardiogram revealed marked dilated right atrium and right ventricle in addition to small and compressed left atrium and left ventricle. RA, right atrium; RV, right ventricle; LA, left atrium; LV, left ventricle.
In view of severe PAH and intractable right heart failure despite maximal medical therapy, she underwent Atrial septostomy (AS) with stenting.
Procedure details
Arterial (5F) and venous access (7F) was obtained, and PA pressures were measured. The pigtail was placed in the posterior sinus to guide the septal puncture. This was then done using brokenbrough needle and mullins sheath was taken into LA. Left upper Pulmonary Vein was wired with 035" Glide wire and 6F Long Sheath was taken across the septum. Left upper Pulmonary Vein was then wired parallelly with 014" Road Runner wire and Glide wire was withdrawn. The atrial septum was subsequently dilated with a 5 mm × 8 cm B Mustang balloon. (Figure 2). Renofit stent (6x12mm) was then taken across the septum and position was confirmed using sheath injection. The stent was then deployed at 12atm. (Figure 3). ECHO and sheath injection showed the stent positioned across the septum.
Transthoracic echocardiogram confirmed the establishment of an inter-atrial shunting from right to left. She was discharged with stable functional II symptoms.
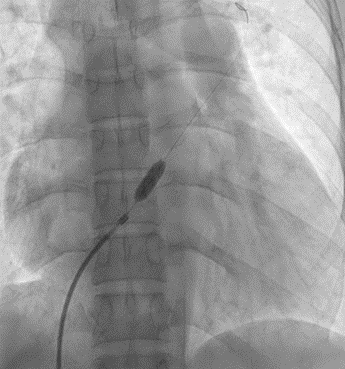
Figure 2: The atrial septum was dilated with a 6 mm × 8 cm balloon (white arrow).
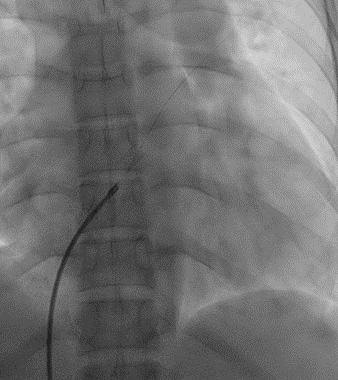
Figure 3: Renofit stent 6x12mm was deployed across the septum
Discussion
PAH is a progressive disease, and, in some cases, patients progress to a point where they are refractory to PAH-specific therapy. Such patients have a high mortality. Lung transplantation is a definitive form of therapy for such cases, even though access might be limited, while the creation of a right-to-left shunt can be recommended as palliative procedure or bridge to transplant.
Atrial septostomy reduces right ventricular filling pressures and increases cardiac output by creating an inter-atrial right to left shunt. Even though this results in arterial desaturation, overall systemic oxygen delivery increases due to increased cardiac output. (5) Patients with pulmonary hypertension and a concomitant patent foramen ovale have better survival outcomes, indicating the potential benefit of such a shunt in the management of pulmonary hypertension (6)
AS is currently indicated for patients with specific criteria that can be considered palliative or bridging.(1,4)
- Severe PAH and intractable right heart failure and those with syncopal episodes (due to diminished cardiac output) despite maximal medical therapy, including optimized PAH specific agents and inotropes.
- Palliation with restoration and maintenance of clinical stability until lung transplantation can be performed (bridge to transplant)
- When no other option exists, for example in regions where modern PAH medical therapy is not available.
It should be kept in mind that one should consider the procedure before any hemodynamic compromise or advanced end-organ dysfunction.
Various studies have shown the benefits of atrial septostomy in these patients. In a case series of 15 patients with refractory primary pulmonary hypertension, atrial septostomy resulted in a 3- year survival rate of 92% compared to 52% in historical controls (7), as well as significant improvements in mean functional status. In another case series of 15 patients with severe pulmonary hypertension and recurrent syncope, there were no further syncopal episodes post procedure (8) and there was an improvement in 3- year survival (65% vs 41% in registry controls)
A systematic review and meta-analysis to determine the evidence supporting the use of BAS in PAH revealed significant reductions in right atrial pressure (–2.77 mm Hg[95% CI, –3.50, –2.04]; P < .001) and increases in cardiac index (0.62 L/min/m2 [95% CI,0.48, 0.75]; P < .001) and left atrial pressure (1.86 mm Hg [95% CI, 1.24, 2.49]; P < .001) following BAS, along with a significant reduction in arterial oxygen saturation (–8.45% [95% CI, –9.93, –6.97]; P < .001) suggesting that BAS is relatively safe in advanced PAH, with beneficial hemodynamic effects.
Based on retrospective analyses examining the outcomes of patients undergoing AS for PAH, several predictors of higher morbidity and mortality with the procedure have been identified. Contraindication for atrial septostomy are the followings (3,9)
- severe RV failure on cardiorespiratory support,
- mean right atrial pressure (mRAP) >20 mm Hg,
- room-air resting O2 saturation < 90>
- left ventricular end diastolic pressure (LVEDP)> 18 mm Hg
The most updated algorithm on the management of PAH recommended that balloon AS should be considered (class II a–c recommendation) in patients who either do not respond to maximal medical therapy or as a bridge to lung transplantation. On the other hand, the United Kingdom’s
National Institute for Health and Clinical Excellence (NICE) failed to mention AS as a potential therapeutic modality.(10)
Although there is scope for further study, such as AS plus medical therapy vs medical therapy alone, our current thought is that this procedure is underutilized, which is probably the reason behind overestimation of its risks and underestimation of its benefits.
In conclusion, it is relatively safe procedure associated with largely favorable hemodynamic outcomes in carefully selected patients with PAH and therapeutic decision for each case should be carefully individualised.
Take Home Messages
- Atrial septostomy is a therapeutic option in patients with severe PAH.
- It is relatively safe procedure associated with largely favorable hemodynamic outcomes in carefully selected patients with PAH.
- Hypoxia is a relative but not an absolute contraindication for atrial septostomy in patients with severe refractory PAH.
- Therapeutic decision for each case should be carefully individualised.
References
- Klepetko W, Mayer E, Sandoval J, Trulock EP, Vachiery JL, Dartevelle P, et al. (2004). Interventional and surgical modalities of treatment for pulmonary arterial hypertension. J Am Coll Cardiol. Jun 16;43(12 Suppl S):73S-80S.
View at Publisher | View at Google Scholar - D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. (1991). Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. Sep 1;115(5):343–349.
View at Publisher | View at Google Scholar - Al Maluli H, DeStephan CM, Alvarez RJ, Sandoval J. (2015). Atrial Septostomy: A Contemporary Review. Clin Cardiol. Mar 2;38(6):395–400.
View at Publisher | View at Google Scholar - Sandoval J, Rothman A, Pulido T. (2001). Atrial septostomy for pulmonary hypertension. Clin Chest Med. Sep;22(3):547–60.
View at Publisher | View at Google Scholar - Reichenberger F, Pepke-Zaba J, McNeil K, Parameshwar J, Shapiro LM. (2003). Atrial septostomy in the treatment of severe pulmonary arterial hypertension. Thorax. Sep;58(9):797–800.
View at Publisher | View at Google Scholar - Rozkovec A, Montanes P, Oakley CM. (1986). Factors that influence the outcome of primary pulmonary hypertension. Br Heart J. May;55(5):449–58.
View at Publisher | View at Google Scholar - Sandoval J, Gaspar J, Pulido T, Bautista E, Martínez-Guerra ML, Zeballos M, et al. (1998). Graded balloon dilation atrial septostomy in severe primary pulmonary hypertension. A therapeutic alternative for patients nonresponsive to vasodilator treatment. J Am Coll Cardiol. Aug;32(2):297–304.
View at Publisher | View at Google Scholar - Kerstein D, Levy PS, Hsu DT, Hordof AJ, Gersony WM, Barst RJ. (1995). Blade balloon atrial septostomy in patients with severe primary pulmonary hypertension. Circulation. Apr 1;91(7):2028–35.
View at Publisher | View at Google Scholar - Bhamra-Ariza P, Keogh AM, Muller DWM. (2014). Percutaneous interventional therapies for the treatment of patients with severe pulmonary hypertension. J Am Coll Cardiol. Feb 25;63(7):611–8.
View at Publisher | View at Google Scholar - Project documents | Drugs for the treatment of pulmonary arterial hypertension [ID12] | Guidance | NICE [Internet]. NICE; 2009 [cited 2024 Apr 18].
View at Publisher | View at Google Scholar
