

Review Article | DOI: https://doi.org/10.31579/2835-8325/138
Anaesthetic Management of a patient of Brugada Syndrome for an Elective Laparoscopic Cholecystectomy- A Case Report
- Somalia Mukherjee *
Apollo Multispeciality Hospital, Kolkata, West Bengal, India.
*Corresponding Author: Somalia Mukherjee. Apollo Multispeciality Hospital, Kolkata, West Bengal, India.
Citation: Somalia Mukherjee, (2024), Anaesthetic Management of a patient of Brugada Syndrome for an Elective Laparoscopic Cholecystectomy- A Case Report, Clinical Research and Clinical Reports, 6(1); DOI: 10.31579/2835-8325/138
Copyright: © 2024, Somalia Mukherjee. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 October 2024 | Accepted: 18 November 2024 | Published: 18 December 2024
Keywords: brugada syndrome; arrhythmogenic right ventricular dysplasia (arvd); malignant dysrhythmia; sudden cardiac death
Abstract
Brugada Syndrome (BrS) is a myocardial transmembrane conduction of sodium abnormality and a common cause of sudden cardiac death (SCD). It is characterized by an ECG pattern of right bundle branch block and ST segment elevation in precordial leads V1–V3. Many factors during general anaesthetic management could precipitate malignant dysrhythmia. We report a case of a patient with incidental diagnosis of BrS posted for elective Laparoscopic Cholecystectomy.
Introduction
Brugada syndrome (BrS) has originally been described in 1992 by Brugada and Brugada as an autosomal-dominant inherited arrhythmic disorder characterized by ST elevation with negative T wave in the right precordial leads without structural cardiac abnormalities [1,2]. The most serious clinical presentation in BrS is sudden cardiac death (SCD) due to ventricular fibrillation (VF), which can be the first manifestation. Some patients present with syncope or can be completely asymptomatic. VF episodes occur predominantly in men, with a 5.5-fold risk of SCD compared with women [3]. BrS is also known as one of the causes for sudden infant death syndrome or SCD in young children [4,5]. The prevalence of BrS is reported to be low in the general population. According to studies in Europe, the incidence of sudden death in the general population is 1.34 per 100 000 per year [6], and ≈5% show no structural heart abnormality [7]. Vagal tone might play a role in arrhythmic events [8-11]. Fever is an important precipitating factor. The diagnostic criteria of BrS consist of 2 parts: (1) detection of the typical ECG abnormality and (2) clinical characteristics [3]. In conjunction with the ECG abnormality, one of the following criteria is necessary: (1) a history of VT (ventricular tachycardia)/VF, (2) a family history of SCD, (3) a family history of coved-type ECG, (4) agonal respiration during sleep, or (5) inducibility of VT/VF during electrophysiological study. BrS can be of three types: Type 1-coved type ST elevation ≥ 2 mm with T inversion. Type 2- ST elevation of < 2mm xss=removed> We report a case of incidentally detected BrS during preoperative assessment posted for laparoscopic cholecystectomy under general anaesthesia.
Case history:
A 56yrs old gentleman with background history of hypothyroidism and seizure disorder was admitted to our hospital with complaints of right sided hypochondriac pain for 1.5 months. There were associated episodes of vomiting, loss of appetite and constipation. Past medical history suggested that the patient is hypothyroid for the past 20 years and is on thyroxine supplementation orally, 150mcg daily. He also had an episode of seizure ~ 10 years back and is on oral phenytoin supplementation 100mg daily since then. He also mentioned of an episode of syncope 2 years back. Past surgical history was noncontributory. However, the patient mentioned to have lost two of his brothers due to SCD, the cause apparently was unknown. Routine blood investigations were acceptable. Recent TSH was 4.5µIU/ml. The lipid profile was however deranged. The patient was reviewed by a neurologist and was advised to continue phenytoin keeping in mind the serious risks of withdrawing long term phenytoin therapy. MRI Brain and EEG were normal. The patient was also reviewed by the gastroenterologist and relevant work up was performed. USG abdomen revealed gall bladder calculi with CBD sludge which was further confirmed on MRCP. The patient was planned for ERCP with CBD clearance followed by cholecystectomy and pre-procedure cardiology clearance was sought. During cardiological evaluation preoperative ECG revealed features suggestive of Type I BrS (as shown in figure 1 and 2). The patient was advised Cardiac MRI to rule out arrhythmogenic right ventricular dysplasia (ARVD) in view of ECG findings, h/o syncope and family h/o sudden deaths. Cardiac MRI showed significantly reduced RVEF (37.8%, N.R:47-74%) with patchy fibrofatty infiltration of the RVOT wall suggestive of Early ARVD. Patient and relatives were counselled regarding the cardiac condition and ICD implantation was advised by the cardiologist to prevent sudden cardiac death. The patient didn’t consent for electrophysiological study and ICD implantation and wanted to proceed for surgery being aware of the very high risk for perioperative major adverse cardiac events (MACE).
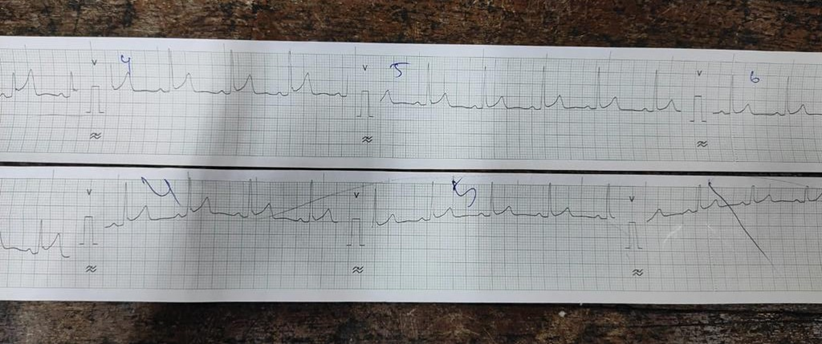
Figure 1: preop ECG of the patient
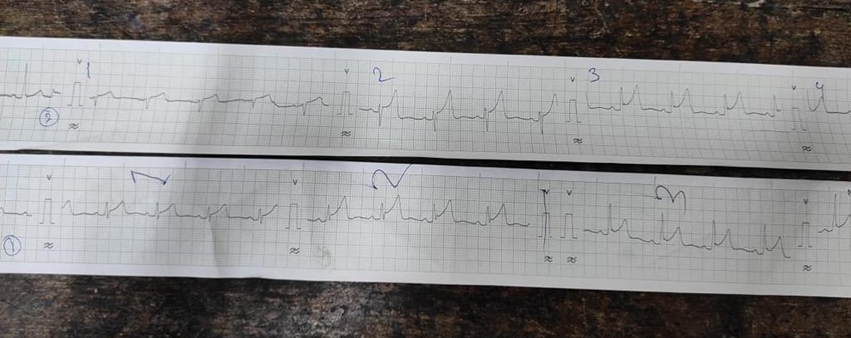
Figure 2: Perioperative anaesthetic management:
Based on clinical examination, investigations and the planned surgical procedure, general anaesthesia was planned. Detailed counselling with patient and relatives was done and high-risk consent for anesthesia and surgery was obtained. Peripheral venous access was obtained with two 18G cannula and an infusion of lactated Ringer’s solution was started. A 20G arterial cannula was inserted into the right radial artery under local anaesthesia and transduced. A three lumen 7.5Fr central venous catheter was inserted into right internal jugular vein under local anesthesia using USG guidance. Disposable transcutaneous defibrillator pads were attached and connected to an external defibrillator before induction. During surgery, electrocardiography, invasive blood pressure, pulse oximetry, end tidal carbon dioxide, temperature, depth of anaesthesia (by etMAC) was continuously recorded. Emergency medications were kept ready. General anaesthesia was induced by intravenous propofol (2mg/kg), fentanyl (2µg/kg) followed by atracurium (0.5mg/kg), before intubation. Mechanical ventilation (Tidal Volume 7 mL/kg, FiO2 50%) was started and targeted to an EtCO2 of 30–35mmHg. The anaesthesia was maintained by sevoflurane with air oxygen mixture to a target etMAC of 0.9-1.0 and supplemental doses of atracurium. Analgesia was provided with intravenous paracetamol 1g, ketorolac 30mg and tramadol 50mg. At the end of the surgery, neostigmine 2.5mg and glycopyrrolate 0.5mg was administered to reverse muscle relaxation. Patient was extubated in the theatre suite uneventfully. Postoperative care was provided in the post anaesthesia care unit. No untoward events (bradycardia or ventricular arrhythmias) occurred during the procedure. Total surgery and anaesthesia duration were 90 minutes. The patient was shifted to the CCU for post-operative cardiac monitoring.
Discussion:
BrS is a congenital cardiac disorder resulting from mutation of the SCN5A gene which encodes for tetrodotoxin insensitive human cardiac voltage gated sodium channels (hH1) [12]. This decreases sodium influx available during phase 0 (upstroke) and 1 (early repolarisation) of cardiac action potential leading to characteristic ST changes in ECG (coved-shaped ST elevation in right precordial leads). Mutations in genes coding for alpha1 and beta2 subunits of L-type calcium channels (CACNA1C and CACNB2) can cause a variant of BrS which causes ST elevation, short QT interval and sudden cardiac death [13]. BrS and ARVD have common pathogenic association due to an unwanted communication between desmosomal and sodium channel proteins. While ARVD is a disorder characterized by loss of right ventricular myocardium with fibrofatty substitution which leads to malignant ventricular arrhythmias. BrS is a primary electrical heart disease, and the ventricular electrical instability is not directly related to any structural myocardial changes. BrS is the most prevalent cause of sudden cardiac death in a young population [3]. The syndrome is familial with an autosomal dominant mode of transmission with incomplete penetrance. Anaesthesiologists routinely use drugs that interact with cardiac ion channels, which can lead to the development of malignant arrhythmias. Previous uneventful general anaesthesia does not lower risks of subsequent adverse events [14, 15]. Some literature supports the avoidance of propofol administration either during induction or continuous infusions in BrS patients. Among volatile anaesthetics, sevoflurane is the one of choice, as it provides greater QT interval stability [16, 17]. Both depolarizing and non-depolarizing NMBA’s can be used without problems. Data regarding the safety of commonly used vasopressors is scarce. Factors that might exacerbate ST-segment elevations and lead to arrhythmias, such as hyperthermia, bradycardia, dyselectrolytaemias like hyper/hypokalaemia and hypercalcemia need correction, as well as autonomic and postural disturbances. Adequate depth of anaesthesia, optimum analgesia, maintenance of homeostasis and continuous monitoring in CCU for at least 24h after surgery are strongly recommended. Experience of general anaesthesia in BrS is still very limited in clinical practice. Patients without ICD should be monitored in a coronary care unit after surgery. In our patient use of propofol and neostigmine did not cause any problems. We didn’t need any vasopressor support perioperatively in our case.
BrS poses a challenge for anaesthesiologists due to possible induction of fatal arrhythmias caused by the common anaesthetic factors such as drugs, temperature variations, hemodynamic & electrolytic alterations and lack of evidence-based guidelines for anaesthetic management of these patients.
References
- Brugada P, Brugada J. (1992), Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol. 20:1391–1396.
View at Publisher | View at Google Scholar - Wilde AA, Antzelevitch C, Borggrefe M, Brugada J, Brugada R, Brugada P. et al. (2002) Proposed diagnostic criteria for the Brugada syndrome: consensus report. Circulation.; 106:2514–2519.
View at Publisher | View at Google Scholar - Antzelevitch C, Brugada P, Borggrefe M, Brugada J, Brugada R, et al (2005) Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation. 659–670.
View at Publisher | View at Google Scholar - Priori SG, Napolitano C, Giordano U, Collisani G, Memmi M. Brugada syndrome and sudden cardiac death in children. Lancet. 2000; 355:808809.
View at Publisher | View at Google Scholar - Probst V, Denjoy I, Meregalli PG, Amirault JC, Sacher F, Mansourati J. et al. Clinical aspects and prognosis of Brugada syndrome in children. Circulation. 2007; 115:2042–2048.
View at Publisher | View at Google Scholar - Behr ER, Dalageorgou C, Christiansen M, Syrris P, Hughes S, Tome Esteban MT. et al. Sudden arrhythmic death syndrome: familial evaluation identifies inheritable heart disease in the majority of families. Eur Heart J. 2008; 29:1670–1680.
View at Publisher | View at Google Scholar - Survivors of out-of-hospital cardiac arrest with apparently normal heart. Need for definition and standardized clinical evaluation. Consensus statement of the Joint Steering Committees of the Unexplained Cardiac Arrest Registry of Europe and of the Idiopathic Ventricular Fibrillatio Registry of the United States. Circulat on.1997; 95:265–272.
View at Publisher | View at Google Scholar - Kasanuki H, Ohnishi S, Ohtuka M, Matsuda N, Nirei T, Isogai. et al. Idiopathic ventricular fibrillation induced with vagal activity in patients without obvious heart disease. Circulation. 1997; 95:2277–2285.
View at Publisher | View at Google Scholar - Agostini D, Scanu P, Loiselet P, Babatasi G, Darlas Y, Grollier G. et al. Iodine-123-metaiodobenzylguanidine SPECT of regional cardiac adrenergic denervation in Brugada syndrome. J Nucl Med. 1998; 39:1129–1132.
View at Publisher | View at Google Scholar - Miyazaki T, Mitamura H, Miyoshi S, Soejima K, Aizawa Y, Ogawa S. Autonomic and antiarrhythmic drug modulation of ST segment elevation in patients with Brugada syndrome. J Am Coll Cardiol. 1996; 27:1061–1070.
View at Publisher | View at Google Scholar - Makimoto H, Nakagawa E, Takaki H, Yamada Y, Okamura H, Noda T et al. Augmented ST-segment elevation during recovery from exercise predicts cardiac events in patients with Brugada syndrome. J Am Coll Cardiol. 2010; 56:1576–1584.
View at Publisher | View at Google Scholar - Rook MB, Bezzina Alshinawi C, Groenewegen WA. Human SCN5A gene mutations alter cardiac sodium channel kinetics and are associated with the Brugada syndrome. Cardiovasc Res. 1999; 44:507-17.
View at Publisher | View at Google Scholar - Antzelevitch C, Cordeire JM, Casio O, Sanguinettti MC, Aizaw Y. Loss of function mutations in cardiac calcium channel underlie a new clinical entity characterised by ST segment elevation, short QT intervals, and sudden cardiac death. Circulation. 2007; 115(4):442-49.
View at Publisher | View at Google Scholar - Brugada P, Brugada J, Brugada R. “Arrhythmia induction by antiarrhythmic drugs,” Pacing and Clinical Electrophysiology,.291–292,2000.
View at Publisher | View at Google Scholar - Postema PG, Wolpert C, Amin AS. “Drugs and Brugada syndrome patients: review of the literature, recommendations, and an up-to-date website (www.brugadadrugs.org),” Heart Rhythm, pp.1335–1341,2009.
View at Publisher | View at Google Scholar - Hayashida H, Miyauchi Y (2006) Anaesthetic management in patients with high-risk Brugada syndrome. Br J Anaesth 97: 118-119.
View at Publisher | View at Google Scholar - Niyazi G, Ismail K, Cengiz BD, Mehmet B, Beyhan E (2001) The effects of volatile anesthetics on the Q-Tc interval. J Cardio Vasc Anesth 15: 188-191.
View at Publisher | View at Google Scholar
