

Research Article | DOI: https://doi.org/10.31579/2835-8147/087
Alzheimer's Disease and the Therapeutic Potential of theta Burst Stimulation: A Systematic Review of Preclinical and Clinical Studies
- Negin Eissazade 1,2*
- Pouria Akbarikoli
- Neguine Rezaii
- Mohammadreza Shalbafan
- Hesam Mosavari
1Cellular and Molecular Research Center, Iran University of Medical Sciences, Tehran, Iran.
2Brain and Cognition Clinic, Institute for Cognitive Sciences Studies, Tehran, Iran.
3Department of Neurology, Massachusetts General Hospital/Harvard Medical School, Boston, Massachusetts, USA.
4Mental Health Research Center, Psychosocial Health Research Institute (PHRI), Department of Psychiatry, School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
5Artificial Intelligence in Health Research Center, Iran University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Negin Eissazade, Cellular and Molecular Research Center, Iran University of Medical Sciences, Tehran, Iran, Brain and Cognition Clinic, Institute for Cognitive Sciences Studies, Tehran, Iran.
Citation: Negin Eissazade, Pouria Akbarikoli, Neguine Rezaii, Mohammadreza Shalbafan, Hesam Mosavari, (2025), Alzheimer's Disease and the Therapeutic Potential of theta Burst Stimulation: A Systematic Review of Preclinical and Clinical Studies, Clinics in Nursing, 4(3); DOI:10.31579/2835-8147/087.
Copyright: © 2025, Negin Eissazade. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 April 2025 | Accepted: 12 May 2025 | Published: 22 May 2025
Keywords: alzheimer’s disease; theta burst stimulation; neuromodulation
Abstract
Alzheimer’s disease (AD) is a progressive neurodegenerative disorder characterized by cognitive decline and behavioral impairment. Despite growing research efforts, effective disease-modifying interventions remain elusive. Theta burst stimulation (TBS), a form of repetitive transcranial magnetic stimulation (rTMS), has shown promise in modulating cortical excitability, synaptic plasticity, and neuroprotective mechanisms. This systematic review aimed to evaluate the efficacy and safety of TBS in AD by synthesizing findings from preclinical and clinical studies.
Methods:
A systematic search of PubMed, Scopus, Embase, Web of Science, and the Cochrane Library was conducted up to January 2025. Studies investigating TBS, including intermittent TBS [iTBS] and continuous TBS [cTBS], in human patients with AD or in animal models of AD were included. Primary outcomes included cognitive function and neuropsychiatric symptoms. Secondary outcomes included biomarkers of neuroplasticity and neurodegeneration. The risk of bias was assessed using the Joanna Briggs Institute (JBI) and Systematic Review Centre for Laboratory Animal Experimentation (SYRCLE) tools.
Results:
Twenty studies met the inclusion criteria, comprising six preclinical and 14 clinical studies. Preclinical evidence suggests that TBS reduces amyloid-beta deposition, enhances synaptic plasticity, mitigates neuroinflammation and oxidative stress, and improves cognitive performance in animal models of AD. iTBS targeting the dorsolateral prefrontal cortex (DLPFC) improved cognitive function, depression, anxiety, and activities of daily living, with some studies reporting non-significant findings in specific neuropsychological assessments. Neuroplasticity changes were observed in motor-evoked potentials and resting motor thresholds, with lower responses in patients with AD and variable reproducibility over time. Additionally, structural and functional brain changes, including preserved hippocampal volume and enhanced frontal beta activity, were associated with cognitive improvements. Adverse events were mild and well- tolerated. Conclusion: Preclinical studies robustly support the neuroprotective and neuropsychiatric effects of TBS in AD models. Clinical findings suggest possible benefits of TBS, particularly iTBS over the DLPFC; however, clinical results are inconsistent and limited by small sample sizes and protocol variability. These findings highlight the challenges of translating animal data to humans and underscore the need for larger, controlled randomized clinical trials to confirm safety and efficacy and optimize treatment parameters.
1.Introduction
Alzheimer's disease (AD) is the leading cause of dementia worldwide, with its prevalence projected to escalate significantly in the coming decades [1]. This progressive neurodegenerative disorder is characterized by cognitive and behavioral deterioration resulting from widespread degenerative changes within the central nervous system [1]. Despite substantial advances in pharmacological research, effective therapies capable of halting or reversing AD progression remain elusive. While new generations of FDA-approved medications have been shown to slow disease progression, they are associated with potentially serious side effects, necessitating careful risk-benefit assessments [2, 3]. Consequently, alternative and complementary treatment modalities are garnering increasing attention [1, 4]. Theta burst stimulation (TBS), a form of repetitive transcranial magnetic stimulation (rTMS), was first introduced in 2005 and has since emerged as a promising intervention for modulating cortical excitability and synaptic plasticity [5, 6]. Unlike traditional rTMS protocols that utilize fixed high- or low-frequency magnetic pulses, TBS delivers stimulation in short bursts, typically around 190 seconds, resulting in prolonged cortical excitability enhancement [7]. TBS mimics the natural activity of the brain during learning, employing bursts of three biphasic pulses at 50 Hz, separated by 5 Hz (200-millisecond intervals) [6]. This innovative design allows for shorter treatment sessions, reduced stimulation intensities, and comparable safety and efficacy to conventional rTMS [5]. TBS can be administered in two primary modes: continuous TBS (cTBS) and intermittent TBS (iTBS). cTBS, delivered over 20–40 seconds, induces long-term depression and reduces cortical excitability, suggesting a possible dependence on NMDA (N-methyl-D-aspartate) receptor activity. In contrast, iTBS is administered in two-second trains interspersed with eight-second intervals, over a total duration of 190 seconds, facilitating long-term potentiation (LTP) and enhancing cortical excitability [5, 6]. Importantly, variations in protocol parameters, such as pulse number, and stimulation site (e.g., dorsolateral prefrontal cortex [DLPFC], primary motor cortex [M1], and cerebellum) can modulate or even reverse the expected effects, highlighting the adaptability of TBS protocols [5, 6, 8, 9]. The clinical applications of TBS, particularly iTBS, have demonstrated transformative potential. While initially validated for treatment-resistant depression [10], iTBS is increasingly recognized for its benefits in neurodegenerative conditions, including AD, Parkinson’s disease, and multiple sclerosis [11, 12]. Furthermore, accelerated iTBS (aiTBS) delivers the same total pulse count across multiple daily sessions, this not only induces long-lasting cortical excitability, but also reduces clinic visits and offers patients quicker relief while maintaining comparable symptom improvement [13-16]. Given its non-invasive nature and capacity to target specific neural substrates, TBS holds significant promise as a novel therapeutic approach in AD. This systematic review aims to comprehensively evaluate the efficacy and safety of TBS in AD by synthesizing evidence from the existing clinical trials and experimental studies.
Materials and methods
The study protocol was registered on the International Prospective Register of Systematic
Reviews (PROSPERO) [ID: CRD42025632613]. The study is reported in accordance with the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [17].
2.1. Eligibility criteria
We used the PICOT framework (Population, Intervention, Comparator, Outcomes, and Timeframe) to structure this review and specifically address the research question: “Is theta burst stimulation safe and effective for improving the symptoms associated with AD?”. Eligible studies included preclinical animal models of AD, such as APP/PS1 transgenic mice and Wistar rats subjected to streptozotocin (STZ) or trimethyltin (TMT)-induced neurodegeneration, as well as human adults diagnosed with probable AD based on established clinical criteria [18-22], some supported by biomarker confirmation. The intervention comprised TBS protocols applied either as standalone treatments or as components of rTMS for therapeutic purposes or physiological assessment. Comparators included wild-type mice matched to APP/PS1 transgenic models, Wistar rats receiving saline injections instead of neurotoxins, placebo or sham stimulation groups exposed to noise or manual handling without active TBS, and, in clinical studies, sham stimulation, standard care, other neuromodulatory interventions, untreated controls, or healthy controls. Outcomes assessed encompassed a broad range of clinical and neurobiological measures evaluated through validated and standardized scales. In preclinical studies, primary outcomes encompassed cognitive and behavioral assessments (e.g., Morris water maze, Y-maze), along with a comprehensive set of cellular and molecular markers, including Aβ deposition, astrocyte and microglial activation (GFAP, Iba1, CD68), neuronal integrity and survival (NeuN, MAP-2), synaptic plasticity (PSD95, SNAP25, SYN1), apoptotic signaling (Caspase-3, Bax/Bcl- 2 ratio, TUNEL), oxidative stress markers (SOD, MDA, GSH), neurotrophic support (BDNF), and glymphatic function (aquaporin-4). In clinical studies, the primary outcomes focused on changes in clinical symptoms measured by standardized clinical scales, including: Activities of Daily Living (ADL); Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog); ALBA Screening Instrument (ASI); Auditory Verbal Learning Test (AVLT); Boston Naming Test (BNT); Clock-Drawing Test (CDT); Clinical Dementia Rating (CDR); Color Trail Test (CTT); Digit Span Test (DST); Hamilton Anxiety Rating Scale (HAMA); Hamilton Depression Rating Scale (HAM-D or HDRS); Hooper Visual Organization Test (HVOT); Judgment of Line Orientation (JLO) test; Logical Memory Test (LMT); Mini-Mental State Examination (MMSE); Montreal Cognitive Assessment (MoCA); Neuropsychiatric Inventory (NPI); Repeatable Battery for the Assessment of Neuropsychological Status (RBANS); Self-Rating Depression Scale (SDS); Stroop Color and Word Test (SCWT); Symbol Digit Modalities Test (SDMT); Trail Making Test (TMT); and Verbal Fluency Test – Semantic and Letter Fluency (VFT-S/L). Other outcomes related to underlying AD pathologies included changes in biomarkers (e.g., BDNF), brain connectivity measures, and electrophysiological assessments of neuronal excitability. The timeframe of assessment varied across studies, covering both acute and longitudinal effects of TBS. Only studies published in English were included. Studies were excluded if they investigated non-Alzheimer’s dementias or unrelated neurological conditions, or lacked original experimental data. Non-primary research publications, including reviews, editorials, commentaries, book chapters, study protocols, and non–peer-reviewed materials such as conference abstracts without full data, were excluded. Additionally, studies were excluded if they failed to report relevant clinical, cognitive, behavioral, neurobiological, or biomarker outcomes measured by validated and standardized instruments. Studies with inadequate methodological rigor or assessed as high risk of bias were also excluded.
2.2. Information sources, search strategy, and study selection
Potentially eligible articles were identified through an electronic search of bibliographic databases (PubMed, Scopus, Embase, Web of Science, and Cochrane Library) in January 2025. No restrictions were applied regarding publication date. The search strategy included the terms “Theta Burst Stimulation,” and “Alzheimer’s Disease,” along with related keywords, which were combined using Boolean operators in the free-text search fields. The detailed search strategy is provided in Supplementary Material 1. Studies were initially screened based on titles and abstracts. Articles that were clearly irrelevant or did not meet the inclusion criteria were excluded. In cases where eligibility was unclear, a full-text review was performed. Additionally, the reference lists of included articles were manually reviewed to identify any potentially relevant studies not captured through the database search; however, this process did not yield any additional articles. Screening, study selection, data extraction, and risk of bias assessment were conducted independently by two reviewers and cross-checked for accuracy. Any discrepancies between reviewers were resolved through discussion, or consultation with a third reviewer.
2.3. Data collection and synthesis
Extracted data included study design, sample size, subject characteristics (e.g., species, strain, age, and sex for animal studies; demographics for clinical studies), details of the TBS protocol (e.g., stimulation parameters and target site), timing of assessments, and the outcomes measured. Given the heterogeneity across study designs, stimulation protocols, and outcome measures, performing a meta-analysis was not feasible.
2.4. Risk of bias assessment
To assess the methodological quality and risk of bias in the included studies, we employed the Joanna Briggs Institute (JBI) critical appraisal checklists, tailored to the specific study designs. Each study was independently evaluated by two reviewers using the relevant JBI tool. For each checklist item, responses were rated as "Yes," "No," "Unclear," or "Not Applicable." An overall quality rating (e.g., low, moderate, or high risk of bias) was then determined based on the number and significance of criteria met [23, 24]. The quality of the included preclinical studies was evaluated using the Systematic Review Centre for Laboratory Animal Experimentation (SYRCLE) [25], adapted from the Cochrane Collaboration Risk of Bias Tool [26].
Results
A total of 5,731 articles were initially identified through the database search. Following title and abstract screening, 40 articles were selected for full-text review. Ultimately, 20 journal articles, comprising six preclinical studies [27-32] and 14 clinical studies [33-46] met the inclusion criteria and were included in the systematic review (Figure 1). The overall quality of the included studies was assessed as fair (Table 1).
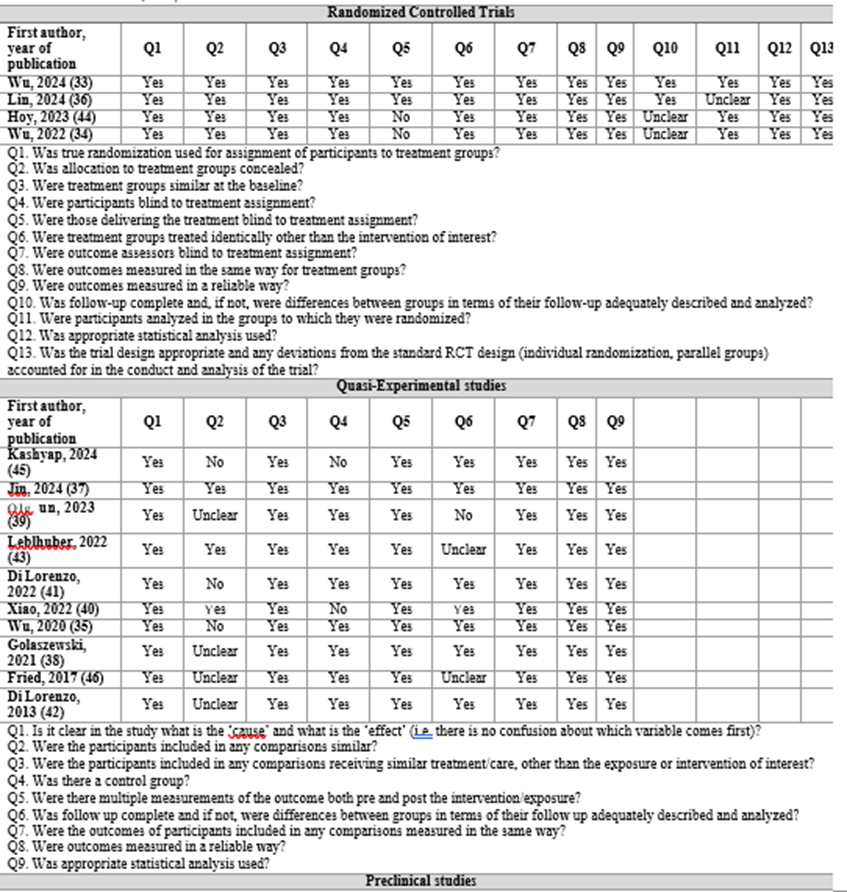
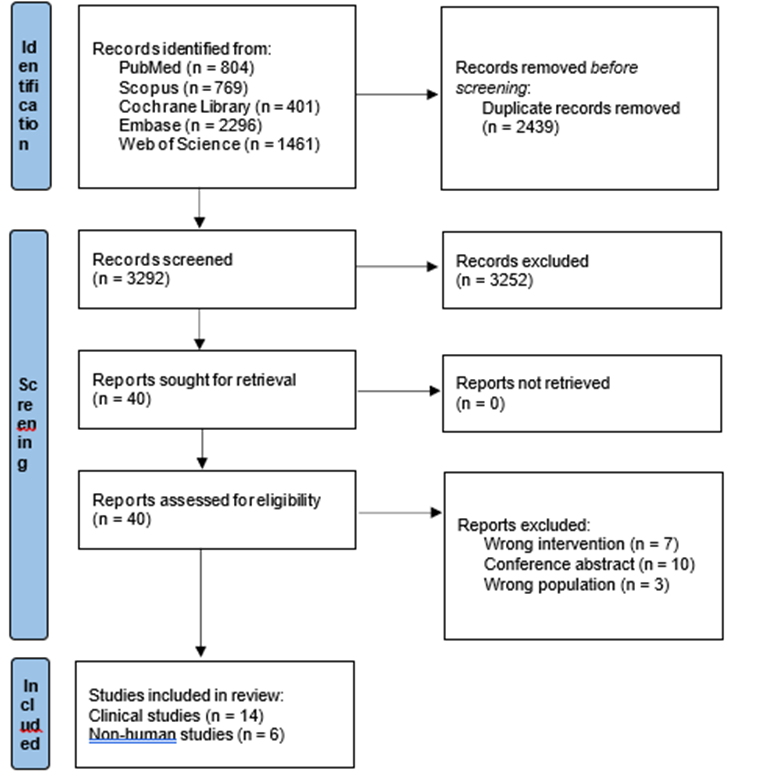
Figure 1: Flow diagram of the included studies
3.1. Preclinical studies
A detailed summary of the animal models, TBS protocols, and assessment time points used in the six included studies is provided in Table 2 [27-32]. Animal studies investigating the effects of TBS on AD have utilized different rodent models, including transgenic APP/PS1 mice (27, 28, 30) and rats with streptozotocin (STZ)-induced [29,31] or trimethyltin (TMT)-induced neurodegeneration (32), replicating key pathological features of AD, such as Aβ accumulation, neuroinflammation, oxidative stress, and cognitive impairment [27-32]. The included studies applied TBS using different stimulation paradigms, varying in the number of trains, pulses per burst, and inter-train intervals. Only one study used cTBS while the other applied iTBS. Stimulation was administered either once daily (28-31) or twice daily [32], over treatment durations ranging from 10 days to one month, with some protocols incorporating breaks between sessions. Stimulation intensities ranged from 33% to 100% of the motor thresholds (MTs). Different coil configurations, including figure-of-eight (25 mm) and circular (60 mm) coils, were employed. Placebo conditions involved noise exposure and manual manipulation without active stimulation. The time of assessment varied across studies, ranging from immediately after TBS treatment [27-29] to follow-up periods of two months post-treatment [30]. One study assessed behavioral outcomes during stimulation periods [32], while others evaluated long-term effects after the final TBS session. Studies consistently demonstrate that TBS exerts neuroprotective effects in AD models by reducing pathological hallmarks, enhancing synaptic plasticity, and improving cognitive function. TBS reduced Aβ burden by downregulating BACE1 (inhibition of Aβ production) and upregulating IDE (facilitation of Aβ degradation) [27, 29, 30]. TBS also promoted glymphatic clearance and improved astrocytic aquaporin-4 (AQP4) polarization, the processes that were correlated with enhanced Aβ removal and cognitive improvements [28]. TBS mitigated neuronal apoptosis, as indicated by decreased expression of pro-apoptotic markers (Caspase-3, Bax) and increased levels of anti-apoptotic and neuronal survival markers (Bcl-2, NeuN) [27, 30, 32]. Synaptic integrity was preserved through increased expression of synaptic proteins, including PSD95, SYN1, SNAP25, and VAMP1, while upregulation of BDNF further supported neuroplasticity (27, 29, 30). Electrophysiological assessments also revealed that TBS enhanced neuronal excitability and reduced hypoactivity in cortical and hippocampal neurons [27]. In addition to neuroprotection, TBS exhibited potent anti-inflammatory and antioxidative effects. Studies reported reductions in microglial and astrocytic activation, as evidenced by decreased expression of Iba1, CD68, and GFAP, along with lower levels of pro-inflammatory cytokines (IL-1β, IL-6, TNF-α, IFN-γ) [27-32]. TBS also restored oxidative balance by enhancing antioxidant enzyme activity (tSOD, MnSOD, GSH) and reducing oxidative stress markers (MDA,3-NT, NO2−) [32]. Furthermore, TBS modulated key signaling pathways involved in cellular survival and synaptic function, including PI3K/Akt/mTOR and ERK1/2, which were restored following stimulation [32].
3.2. Clinical studies
An overview of the 14 clinical studies included in this review is provided in Table 3 [33-46]. Collectively, these studies included 324 patients with AD, and 269 controls. TBS protocols varied in terms of stimulation targets, frequency, duration, and assessment time points. Most studies applied iTBS or accelerated iTBS (aiTBS) over the left DLPFC [33, 36-38,40, 44], with others targeting other brain regions such as the primary motor cortex [39], medial prefrontal cortex [43], and cerebellum [41, 42]. Stimulation intensity ranged from 70% to 100% of the motor threshold (MT), with total pulses varying from 600 and 24,000. Protocols typically involved daily or multiple daily sessions over a period of 5 to 14 days, with follow-up assessments ranging from immediately post-treatment to several months. Sham protocols consistently mimicked auditory and tactile sensations without delivering active stimulation.
3.2.1. DLPFC
iTBS was found to significantly improve cognitive function as measured by MoCA [33, 35, 36,40], MMSE [33, 35, 37, 40], associative memory [35], CDT [35, 38, 40], VFT-S/L [33, 35], BNT[33, 35, 40], DST [35, 40], AVLT [33, 35, 36, 40], SDMT, CTT-RT-B, HVOT, JLOT, LMT [35], and SCWT [40], depression as measured by SDS [37] and HAMD [33, 35, 37, 40], anxiety assessed through HAMA [35, 40], ADL [33, 35, 40], NPI [35, 40], and overall treatment effectiveness (recovery, effectual, in Force, and null and void) [37]. However, some studies reported non-significant findings across NPI (total score, caregiver distress), CTT-RT-A [35], Global Deterioration Scale [33, 40], CDR, Stroop Interference test, TMT A/B, and VFT-animal [40], Geriatric Depression Scale, ADAS-Cog, and quality of life (self, carer) [44]. aiTBS significantly improved associative memory, MMSE, ADL, HAMA, HAMD, LMT- Immediate/Delay, DST-F/B, SDMT, BNT, VFT-S/L, SCWT-Dot, CDT, HVOT, and JLOT scores [34], MoCA, AVLT-Immediate/Delay/Recognition scores [34, 36], and the RBANS attention index [45]. Also, following treatment, there was a trend toward the improvement of story memory which is a part of the immediate memory index [45]. No significant changes were found in anomaly burden, or other RBANS indices (total, immediate memory, visuospatial/constructional, language, delayed memory) [45]. Also, non-significant findings were reported across MMSE, TMT, DST [36], Geriatric Depression Scale [45], NPI, SCWT- word/color word, and CTT-A/B scores [34]. Regarding brain connectivity, iTBS significantly reduced the abnormally elevated connection between the target and right precuneus cortex, which significantly correlated with improvements in VFT-S scores [47]. Moreover, the predictors of change in delayed recall post-iTBS were baseline gamma connectivity (i.e., higher gamma connectivity at baseline predicting greater change in delayed recall) and change in gamma connectivity (i.e., greater change in gamma connectivity predicting greater change in delayed recall) [44]. Significant changes in global mean field amplitude values (P30 and P70) were found post-iTBS, predominantly located at the left frontal region. Furthermore, total MoCA and MMSE scores were inversely correlated with cortical-evoked activity in the DLPFC. Changes in beta oscillations, also concentrated in the left frontal region, were observed [36]. In terms of gray matter volume (GMV), the left and right hippocampal volumes were preserved in the active treatment group but significantly declined in the sham group. Increases in left and right hippocampal GMV were positively correlated with improvements in MoCA and MMSE scores. Also, left hippocampal GMV increases were negatively correlated with Global Deterioration Scale scores, while right hippocampal GMV increases were positively correlated with VFT-S scores. MoCA scores one year after DLPFC-iTBS treatment significantly improved in non-Apolipoprotein E epsilon 4 (ApoE ε4) carriers, with no such improvements in ApoE ε4 carriers. Improvements in CDT performance were also more pronounced in non-ApoE ε4 carriers, with no significant changes noted in other neuropsychological assessments [33].
3.2.2. M1
Regarding neuroplasticity, the percentage amplitude changes of motor evoked potentials (MEPs) and rMTs were significantly lower in patients with AD, compared to healthy controls, and showed no significant correlation with MMSE, ALBA, CDR, or Global Deterioration Scale scores [39]. Another study reported a lower increase in rMT and MEP amplitude at 5 minutes post-iTBS in patients with AD. High reproducibility was observed at 10 minutes post-iTBS, as well as for the total area under the curve during the first 20 minutes following stimulation (AUC –), which corresponds to the typical peak effect period seen in neurotypical individuals. In contrast, only moderate reproducibility was noted at the 5-, 20-, 30-, and 40-minute time points. By 50 minutes post-iTBS, thesed changes were found to be non-reproducible [46].
3.2.3. Medial prefrontal cortex (mPFC)
iTBS over the mPFC significantly improved MMSE (modified repeat address phrase test), 7- item HAMD, and the 6-Item Cognitive Impairment test scores. No significant changes were observed in CDT scores. A trend toward lower serum phenylalanine concentrations was noted [43].
3.2.4. Cerebellum
Two studies targeted the right lateral cerebellum, and subsequently, the posterior and superior
lobules. One study indicated a reduction in MEP amplitude 10 minutes after cTBS in both patients and healthy controls, suggesting motor cortex activity suppression. Conversely, iTBS significantly increased MEP amplitude at 10 and 20 minutes post-stimulation, but only in healthy controls [41]. Another study found that cTBS significantly increased short-latency afferent inhibition (SLAI) in patients with AD at inter-stimulus intervals (ISIs) of 0 ms and +4 ms, with no effects on rMT, intracortical inhibition (SICI) or intracortical facilitation (ICF) in either group [42].
3.2.5. Adverse events
Overall, the procedure was well-tolerated, with the exception of two participants who could not endure the full stimulation intensity and discontinued treatment [45]. Reported adverse events in the active treatment groups included scalp painful discomfort (N = 9) (33, 34, 36, 47), eyelid twitches (N = 5) (34, 36), headache (N = 2), tingling (N = 2), burning pain (N = 1), palpitation (N = 1) (41), and altered consciousness between treatment sessions (N = 1) [45].
Discussion
This systematic review demonstrates the promise of TBS in the treatment of AD, integrating evidence from both preclinical and clinical studies. Of particular importance is the potential of TBS to improve cognitive functioning, as most treatment modalities, at best, only slow the rate of decline. Preclinical studies demonstrated that TBS exerts neuroprotective effects by reducing Aβ burden, enhancing synaptic plasticity, alleviating neuroinflammation and oxidative stress, and improving cognitive function. In clinical studies, TBS, primarily in the form of iTBS or aiTBS targeting DLPFC, was associated with improvements in cognitive function, depression, anxiety, and activities of daily living. Functional and structural neuroimaging findings indicated that TBS modulates brain connectivity and preserves hippocampal volume. Notably, TBS was generally well-tolerated, with only minor adverse events, such as scalp discomfort and headaches reported.Stimulation of different brain regions with TBS yielded distinct cognitive and neurophysiological outcomes. DLPFC-iTBS consistently improved global cognition, memory, and executive function while modulating network connectivity [33-35, 37, 38, 40, 44, 45]. Specifically, iTBS improved functional connectivity between left DLPFC and bilateral caudate, as well as between the right amygdala and right caudate, regions implicated in spatial attention, working memory, and decision-making [48, 49]. These effects may be mediated by excitatory modulation of the prefrontal cortex–a central hub in frontal-limbic circuits. TBS may also support neuronalfunction by enhancing cerebral metabolism, promoting cortical-subcortical interactions, and preserving structural integrity, contributing to cognitive improvements and symptomatic relief in patients with AD [35, 37]. M1-iTBS, though less studied, highlighted impaired motor plasticity in AD, suggesting dysfunction in sensorimotor networks [39, 46]. Moreover, LTP-like plasticity demonstrated moderate reproducibility among patients with AD, suggesting that the pathological processes underlying AD may simultaneously alter and stabilize TMS measures [46]. However, variability in LTP-like plasticity among patients and protocols complicates interpretation of these findings. mPFC-iTBS enhanced cognition and mood, likely by modulating limbic-cognitive circuits, though its effects on executive function remains unclear [43]. Additionally, TBS may impact motor and cognitive processes via cerebellar–cerebral pathways [50, 51], likely involving modulation of Purkinje cells and the dentate nucleus [52-56]. However, findings from cerebellar TBS were mixed: cTBS suppressed, and iTBS enhanced, motor cortex excitability in healthy controls, whereas responses in patients with AD were blunted [41, 42]. These findings highlight the region-specific neuroplasticity deficits in AD, with DLPFC-iTBS remaining the most promising target for cognitive enhancement. Building on this, comparisons among protocols further underscore how differences in stimulation parameters, such as intensity, frequency, spacing, and cortical target, significantly influence treatment efficacy. For instance, two studies administered high-frequency aiTBS over the left DLPFC with twice and three daily sessions, respectively, leading to notable improvements in global cognition and memory, with Wu’s regimen demonstrating sustained benefits at 10 weeks [34, 36]. In contrast, Kashyap et al. (2024) employed a lower daily dose across individualized prefrontal targets and observed improvements limited to attentional domains [45]. These findings underscore that TBS protocols vary in efficacy depending on stimulation parameters such as dosing schedule and target selection. Optimizing these factors is crucial for achieving specific therapeutic outcomes, reinforcing the importance of individualized protocol design and precise anatomical targeting to maximize cognitive benefits in AD. In preclinical studies, iTBS has been shown to mitigate oxidative stress, reduce Aβ and amyloid precursor protein levels, and decrease reactive astrogliosis [29]. TBS exerts multifaceted effects by modulating neurotransmitter systems, particularly GABA and glutamate, and influencing the activity of NMDA and AMPA receptors [57-59]. Furthermore, TBS enhances the expression of BDNF, a critical mediator of neuroplasticity and neuronal survival [60, 61]. Notably, TBS has been associated with reduced expression of CD68 [27, 30], a marker of microglial activation involved in lysosomal Aβ degradation [62]; thus, whether reduced CD68 expression should be interpreted as a favorable outcome of TBS requires further investigation. Collectively, these mechanisms underscore the therapeutic potential of iTBS in fostering neuroprotection and cognitive enhancement, positioning it as a potential strategy to decelerate AD progression [12]. Although preclinical studies robustly demonstrated the efficacy of TBS in animal models of AD, the findings from clinical studies were comparatively inconsistent and less conclusive. This discrepancy underscores the challenges in translating experimental success into clinical effectiveness and highlights the need for more rigorous human research. Moreover, although preclinical studies provided valuable mechanistic insights, the translational value of animal models is inherently limited. Rodent models only partially replicate the multifactorial pathology and chronic progression of human AD, and those induced by neurotoxins (e.g., STZ or TMT) may not accurately reflect sporadic AD pathophysiology. Several limitations further constrain the interpretability and generalizability of the current evidence. First, the relatively small number of included studies and limited sample sizes, particularly in clinical trials, reduce statistical power. Several reported outcomes were derived from single studies with small cohorts and thus require replication in larger, well-powered, multi-center trials. Second, heterogeneity in study designs, including differences in study designs, TBS protocols (e.g., stimulation intensity, number of pulses, session frequency), targeted brain regions, and outcome measures, precluded quantitative meta-analysis and complicated cross study comparisons. This variability also limits the identification of optimal stimulation parameters for specific therapeutic goals. Third, the predominant focus on the DLPFC may introduce bias, as the effects of stimulating other potentially relevant brain regions remain underexplored. Region-specific neuroplasticity responses, especially involving the cerebellum, motor cortex, and medial prefrontal cortex, were insufficiently studied, highlighting a gap in anatomical targeting research. Fourth, short follow-up periods in most studies also limit conclusions about the durability of therapeutic effects. Fifth, there was no consistent reporting on whether AD diagnoses were based on biomarker evidence or clinical judgment alone, a factor that significantly impacts the generalizability and interpretability of findings. Future large-scale, multi-center trials should focus on optimizing stimulation protocols, exploring individualized approaches, and assessing long-term clinical outcomes to advance the clinical application of TBS in AD.
Conclusions
TBS is a non-invasive neuromodulation technique that may hold potential for AD, with preliminary evidence suggesting possible benefits for cognitive function and neuroplasticity. Although the DLPFC is the most frequently targeted region, early findings from stimulation of other areas such as the mPFC, M1, and cerebellum warrant further exploration. Given that current conclusions are primarily based on a limited number of studies, in cases, single studies, more rigorous, large-scale research is needed to clarify the mechanisms, efficacy, and clinical relevance of TBS in AD.
List of abbreviation
Aβ: Amyloid-beta; AD: Alzheimer's disease; ADAS-Cog: Alzheimer's Disease Assessment Scale-Cognitive Subscale; ADL: Activities of Daily Living; Akt: Protein kinase B; AMPA: α- amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; APP: Amyloid precursor protein; AVLT: Auditory Verbal Learning Test; BACE1: β-Site amyloid precursor protein cleaving enzyme 1; BDNF: Brain-derived neurotrophic factor; BNT: Boston Naming Test; CD68: Cluster of differentiation 68; CDR: Clinical Dementia Rating; CDT: Clock-Drawing Test; cTBS: Continuous theta burst stimulation; DLPFC: Dorsolateral prefrontal cortex; DST: Digit Span Test; ERK1/2: Extracellular signal-regulated kinases 1 and 2; GFAP: Glial fibrillary acidic protein; GMV: Gray matter volume; GSH: Glutathione; HAMA: Hamilton Anxiety Scale; HAMD/HDRS: Hamilton Depression Rating Scale; Iba1: Ionized calcium-binding adapter molecule 1; ICF: Intracortical facilitation; IDE: Insulin-degrading enzyme; IFN-γ: Interferon-gamma; IL-1β: Interleukin-1 beta; IL-6: Interleukin-6; iTBS: Intermittent theta burst stimulation; JBI: Joanna Briggs Institute; M1: Primary motor cortex; MDA: Malondialdehyde; MEP: Motor evoked potential; MnSOD: Manganese superoxide dismutase; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; mTOR: Mammalian target of rapamycin; NeuN: Neuronal nuclei; NMDA: N-methyl-D-aspartate; NPI: Neuropsychiatric Inventory; NO2−: Nitrite; PI3K: Phosphoinositide 3-kinase; PROSPERO: International Prospective Register of Systematic Reviews; PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PSD95: Postsynaptic density protein 95; QoL-AD: Quality of Life in Alzheimer's Disease; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; rMT: Resting motor threshold; rTMS: Repetitive transcranial magnetic stimulation; SCWT: Stroop Color-Word Test; SICI: Short-interval intracortical inhibition; SLAI: Short-latency afferent inhibition; SNAP25: Synaptosomal-associated protein 25; SYRCLE: Systematic Review Centre for Laboratory Animal Experimentation; SYN1: Synapsin-1; TBS: Theta burst stimulation; TMT: Trail Making Test; TNF-α: Tumor necrosis factor-alpha; tSOD: Total superoxide dismutase; VAMP1: Vesicle-associated membrane protein 1; VFT: Verbal Fluency Test.
Declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Availability of data and materials
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study, which was conducted as a systematic review.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Authors' contributions
Conceptualization: NE, HM and PA; Data curation: NE, HM and PA; Methodology: NE and HM; Project administration: NE, HM, and PA; Supervision: MSH and NR; Validation: MSH and NR; Writing - original draft; NE, HM and PA; and Writing - review & editing: NE, HM, PA, NR, and MSH. All authors have read and approved the submitted manuscript.
Acknowledgements
The authors would like to thank Professor Mohammad Rohani for his invaluable support and insightful guidance.
References
- Vejandla B, Savani S, Appalaneni R, Veeravalli RS, Gude SS. Alzheimer's Disease: The Past, Present, and Future of a Globally Progressive Disease. Cureus. 2024;16(1):e51705. 10.7759/cureus.51705. van Dyck CH, Swanson CJ, Aisen P, Bateman RJ, Chen C, Gee M, et al. Lecanemab in Early Alzheimer's Disease. N Engl J Med. 2023;388(1):9-21. 10.1056/NEJMoa2212948. Sims JR, Zimmer JA, Evans CD, Lu M, Ardayfio P, Sparks J, et al. Donanemab in Early Symptomatic Alzheimer Disease: The TRAILBLAZER-ALZ 2 Randomized Clinical Trial. Jama. 4692023;330(6):512-27. 10.1001/jama.2023.13239. 4. Cummings J, Zhou Y, Lee G, Zhong K, Fonseca J, Cheng F. [Not Available]. Alzheimers Dement (N Y). 2024;10(2):e12465. 10.1002/trc2.12465. 5. Cole E, O'Sullivan SJ, Tik M, Williams NR. Accelerated Theta Burst Stimulation: Safety, Efficacy, and Future Advancements. Biol Psychiatry. 2024;95(6):523-35 10.1016/j.biopsych.2023.12.004. 6. Huang YZ, Edwards MJ, Rounis E, Bhatia KP, Rothwell JC. Theta burst stimulation of the human motor cortex. Neuron. 2005;45(2):201-6. 10.1016/j.neuron.2004.12.033. 7. Yamaguchi T, Fujiwara T, Lin SC, Takahashi Y, Hatori K, Liu M, et al. Priming With Intermittent Theta Burst Transcranial Magnetic Stimulation Promotes Spinal Plasticity Induced by Peripheral Patterned Electrical Stimulation. Front Neurosci. 2018;12:508.10.3389/fnins.2018.00508. 8. Gamboa OL, Antal A, Moliadze V, Paulus W. Simply longer is not better: reversal of theta burst after-effect with prolonged stimulation. Exp Brain Res. 2010;204(2):181-7.10.1007/s00221-010-2293-4. 9. Huang YZ, Chen RS, Rothwell JC, Wen HY. The after-effect of human theta burst stimulation is NMDA receptor dependent. Clin Neurophysiol. 2007;118(5):1028-32.10.1016/j.clinph.2007.01.021. 10. Cohen SL, Bikson M, Badran BW, George MS. A visual and narrative timeline of US FDA milestones for Transcranial Magnetic Stimulation (TMS) devices. Brain Stimul. 2022;15(1):73-5. 10.1016/j.brs.2021.11.010. 11. Rounis E, Huang YZ. Theta burst stimulation in humans: a need for better understanding effects of brain stimulation in health and disease. Exp Brain Res. 2020;238(7-8):1707-14.10.1007/s00221-020-05880-1. 12. Sharbafshaaer M, Cirillo G, Esposito F, Tedeschi G, Trojsi F. Harnessing Brain Plasticity: The Therapeutic Power of Repetitive Transcranial Magnetic Stimulation (rTMS) and Theta Burst Stimulation (TBS) in Neurotransmitter Modulation, Receptor Dynamics, and Neuroimaging for Neurological Innovations. Biomedicines. 2024;12(11). 10.3390/biomedicines12112506. 13. Dragon K, Janthur C, Hebel T, Abdelnaim MA, Reißmann A, Langguth B, et al. Four weeks standard vs. one week accelerated intermittent Theta Burst Stimulation for the treatment of depression – A retrospective analysis. Behavioural Brain Research. 2025;479:115361. https://doi.org/10.1016/j.bbr.2024.115361. 14. Zhang M, Li W, Hu Z, Lu H, Zhou Y, Ning Y. Antidepressant response time across intermittent theta burst stimulation regimens and efficacy indicators in adolescents depression: a secondary analysis from a randomized controlled trial. BMC Psychiatry. 2024;24(1):905. 10.1186/s12888-024-06346-2. 15. Yu F, Tang X, Hu R, Liang S, Wang W, Tian S, et al. The After-Effect of Accelerated Intermittent Theta Burst Stimulation at Different Session Intervals. Front Neurosci. 2020;14:576. 10.3389/fnins.2020.00576. 16. Hodkinson DJ, Drabek MM, Horvath S, Pszczolkowski S, Tench C, Tanasescu R, et al. Accelerated intermittent theta burst transcranial magnetic stimulation of the dorsolateral prefrontal cortex for chronic knee osteoarthritis pain. Clin Neurophysiol. 2025.10.1016/j.clinph.2025.02.267. 17. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. 2021;372:n71. 10.1136/bmj.n71. 18. Varma AR, Snowden JS, Lloyd JJ, Talbot PR, Mann DM, Neary D. Evaluation of the NINCDS-ADRDA criteria in the differentiation of Alzheimer's disease and frontotemporal dementia. J Neurol Neurosurg Psychiatry. 1999;66(2):184-8. 10.1136/jnnp.66.2.184. 19. Martorana A, Esposito Z, Di Lorenzo F, Giacobbe V, Sancesario GM, Bucchi G, et al. Cerebrospinal fluid levels of Aβ42 relationship with cholinergic cortical activity in Alzheimer's disease patients. J Neural Transm (Vienna). 2012;119(7):771-8. 10.1007/s00702-012-0780-4. 20. McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Jr., Kawas CH, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7(3):263-9. 10.1016/j.jalz.2011.03.005. 21. McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology. 1984;34(7):939-44. 10.1212/wnl.34.7.939. 22. Jack CR, Jr., Albert MS, Knopman DS, McKhann GM, Sperling RA, Carrillo MC, et al. Introduction to the recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement.2011;7(3):257-62. 10.1016/j.jalz.2011.03.004. 23. Barker TH SJ, Sears K, Klugar M, Tufanaru C, Leonardi-Bee J, Aromataris E, Munn Z. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evidence Synthesis. 2023;21(3):494-506. 24. Barker TH HN, Aromataris E, Stone JC, Leonardi-Bee J, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias quasi-experimental studies. JBI Evid Synth 2024;22(3):378-88. 25. Hooijmans CR, Rovers MM, de Vries RBM, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLE’s risk of bias tool for animal studies. BMC Medical Research Methodology. 2014;14(1):43. 10.1186/1471-2288-14-43. 26. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. Bmj. 2011;343:d5928.10.1136/bmj.d5928. 27. Zhu Y, Huang H, Chen Z, Tao Y, Liao LY, Gao SH, et al. Intermittent Theta Burst Stimulation Attenuates Cognitive Deficits and Alzheimer's Disease-Type Pathologies via ISCA1-Mediated Mitochondrial Modulation in APP/PS1 Mice. Neurosci Bull. 2024;40(2):182-200.10.1007/s12264-023-01098-7. 28. Wu C, Lin T, Ding Q, Zhang N, Ou ZT, Cai GY, et al. Continuous Theta-Burst Stimulation Promotes Paravascular CSF-Interstitial Fluid Exchange through Regulation of Aquaporin-4 Polarization in APP/PS1 Mice. Mediators Inflamm. 2022;2022:2140524. 10.1155/2022/2140524. 29. Stanojevic JB, Zeljkovic M, Dragic M, Stojanovic IR, Ilic TV, Stevanovic ID, et al. Intermittent theta burst stimulation attenuates oxidative stress and reactive astrogliosis in the streptozotocin-induced model of Alzheimer's disease-like pathology. Front Aging Neurosci.2023;15:1161678. 10.3389/fnagi.2023.1161678. 30. Huang H, Zhu Y, Liao L, Gao S, Tao Y, Fang X, et al. The long-term effects of intermittent theta burst stimulation on Alzheimer's disease-type pathologies in APP/PS1 mice. Brain Res Bull. 2023;202:110735. 10.1016/j.brainresbull.2023.110735. 31. Stanojevic J, Dragic M, Stevanovic I, Ilic T, Stojanovic I, Zeljkovic M, et al. Intermittent theta burst stimulation ameliorates cognitive impairment and hippocampal gliosis in the Streptozotocin-induced model of Alzheimer's disease. Behav Brain Res. 2022;433:113984.10.1016/j.bbr.2022.113984. 32. Stekic A, Zeljkovic M, Zaric Kontic M, Mihajlovic K, Adzic M, Stevanovic I, et al. Intermittent Theta Burst Stimulation Ameliorates Cognitive Deficit and Attenuates Neuroinflammation via PI3K/Akt/mTOR Signaling Pathway in Alzheimer's-Like Disease Model. Front Aging Neurosci. 2022;14:889983. 10.3389/fnagi.2022.889983. 33. Wu X, Yan Y, Hu P, Wang L, Wu Y, Wu P, et al. Effects of a periodic intermittent theta burst stimulation in Alzheimer's disease. Gen Psychiatr. 2024;37(1):e101106. 10.1136/gpsych-2023-101106. 34. Wu X, Ji GJ, Geng Z, Wang L, Yan Y, Wu Y, et al. Accelerated intermittent theta-burst stimulation broadly ameliorates symptoms and cognition in Alzheimer's disease: A randomized controlled trial. Brain Stimul. 2022;15(1):35-45. 10.1016/j.brs.2021.11.007. 35. Wu X, Ji G-J, Geng Z, Zhou S, Yan Y, Wei L, et al. Strengthened theta-burst transcranial magnetic stimulation as an adjunctive treatment for Alzheimer’s disease: An open-label pilot study. Brain Stimulation: Basic, Translational, and Clinical Research in Neuromodulation.2020;13(2):484-6. 10.1016/j.brs.2019.12.020. 36. Lin H, Liang J, Wang Q, Shao Y, Song P, Li S, et al. Effects of accelerated intermittent theta- burst stimulation in modulating brain of Alzheimer's disease. Cereb Cortex. 2024;34(3).10.1093/cercor/bhae106. 37. Jin X, Xu CY, Fei JF, Fang Y, Sun CH. Alzheimer's disease with depressive symptoms: Clinical effect of intermittent theta burst stimulation repetitive transcranial magnetic stimulation. World J Psychiatry. 2024;14(8):1216-23. 10.5498/wjp.v14.i8.1216. 38. Golaszewski S, Kunz A, Schwenker K, Sebastianelli L, Versace V, Ferrazzoli D, et al. Effects of Intermittent Theta Burst Stimulation on the Clock Drawing Test Performances in Patients with Alzheimer's Disease. Brain Topogr. 2021;34(4):461-6. 10.1007/s10548-021-00836-2. 39. Olğun Y, Aksoy Poyraz C, Bozluolçay M, Gündüz A, Poyraz B. A comparative transcranial magnetic stimulation study: Assessing cortical excitability and plasticity in Alzheimer's disease, dementia with Lewy bodies and Frontotemporal dementia. Psychogeriatrics. 2024;24(2):272-80.10.1111/psyg.13070. 40. Xiao G, Wu Y, Yan Y, Gao L, Geng Z, Qiu B, et al. Optimized Magnetic Stimulation Induced Hypoconnectivity Within the Executive Control Network Yields Cognition Improvements in Alzheimer's Patients. Front Aging Neurosci. 2022;14:847223. 10.3389/fnagi.2022.847223. 41. Di Lorenzo F, Bonni S, Picazio S, Motta C, Caltagirone C, Martorana A, et al. Effects of Cerebellar Theta Burst Stimulation on Contralateral Motor Cortex Excitability in Patients with Alzheimer's Disease. Brain Topogr. 2020;33(5):613-7. 10.1007/s10548-020-00781-6. 42. Di Lorenzo F, Martorana A, Ponzo V, Bonni S, D'Angelo E, Caltagirone C, et al. Cerebellar theta burst stimulation modulates short latency afferent inhibition in Alzheimer's disease patients. Front Aging Neurosci. 2013;5:2. 10.3389/fnagi.2013.00002. 43. Leblhuber F, Geisler S, Ehrlich D, Steiner K, Kurz K, Fuchs D. High Frequency Repetitive Transcranial Magnetic Stimulation Improves Cognitive Performance Parameters in Patients with Alzheimer's Disease - An Exploratory Pilot Study. Curr Alzheimer Res. 2022;19(9):681-8.10.2174/1567205019666220920090919. 44. Hoy KE, Emonson MRL, Bailey NW, Rogers C, Coyle H, Stockman F, et al. Gamma connectivity predicts response to intermittent theta burst stimulation in Alzheimer's disease: a randomized controlled trial. Neurobiol Aging. 2023;132:13-23.10.1016/j.neurobiolaging.2023.08.006. 45. Kashyap B, Hanson LR, Gustafson SK, Barclay T, Howe CM, Sherman SJ, et al. Open label pilot of personalized, neuroimaging-guided theta burst stimulation in early-stage Alzheimer's disease. Front Neurosci. 2024;18:1492428. 10.3389/fnins.2024.1492428. 46. Fried PJ, Jannati A, Davila-Perez P, Pascual-Leone A. Reproducibility of Single-Pulse, Paired-Pulse, and Intermittent Theta-Burst TMS Measures in Healthy Aging, Type-2 Diabetes, and Alzheimer's Disease. Front Aging Neurosci. 2017;9:263. 10.3389/fnagi.2017.00263. 47. Wu X, Ji GJ, Geng Z, Zhou S, Yan Y, Wei L, et al. Strengthened theta-burst transcranial magnetic stimulation as an adjunctive treatment for Alzheimer's disease: An open-label pilot study. Brain Stimul. 2020;13(2):484-6. 10.1016/j.brs.2019.12.020. 48. Chu M, Zhang Y, Chen J, Chen W, Hong Z, Zhang Y, et al. Efficacy of Intermittent Theta- Burst Stimulation and Transcranial Direct Current Stimulation in Treatment of Post-Stroke Cognitive Impairment. J Integr Neurosci. 2022;21(5):130. 10.31083/j.jin2105130. 49. Alkhasli I, Sakreida K, Mottaghy FM, Binkofski F. Modulation of Fronto-Striatal Functional Connectivity Using Transcranial Magnetic Stimulation. Front Hum Neurosci. 2019;13:190.10.3389/fnhum.2019.00190. 50. Toniolo S, Serra L, Olivito G, Marra C, Bozzali M, Cercignani M. Patterns of Cerebellar Gray Matter Atrophy Across Alzheimer's Disease Progression. Front Cell Neurosci. 2018;12:430.10.3389/fncel.2018.00430. 51. Toniolo S, Serra L, Olivito G, Caltagirone C, Mercuri NB, Marra C, et al. Cerebellar White Matter Disruption in Alzheimer's Disease Patients: A Diffusion Tensor Imaging Study. J Alzheimers Dis. 2020;74(2):615-24. 10.3233/jad-191125. 52. Evans GJ. Synaptic signalling in cerebellar plasticity. Biol Cell. 2007;99(7):363-78.10.1042/bc20070010. 53. Koch G, Mori F, Marconi B, Codecà C, Pecchioli C, Salerno S, et al. Changes in intracortical circuits of the human motor cortex following theta burst stimulation of the lateral cerebellum. Clin Neurophysiol. 2008;119(11):2559-69. 10.1016/j.clinph.2008.08.008. 54. Wu T, Hallett M. The cerebellum in Parkinson's disease. Brain. 2013;136(Pt 3):696-709.10.1093/brain/aws360. 55. Daskalakis ZJ, Paradiso GO, Christensen BK, Fitzgerald PB, Gunraj C, Chen R. Exploring the connectivity between the cerebellum and motor cortex in humans. J Physiol. 2004;557(Pt2):689-700. 10.1113/jphysiol.2003.059808. 56. Dum RP, Strick PL. An unfolded map of the cerebellar dentate nucleus and its projections to the cerebral cortex. J Neurophysiol. 2003;89(1):634-9. 10.1152/jn.00626.2002. 57. Brown JC, Higgins ES, George MS. Synaptic Plasticity 101: The Story of the AMPA Receptor for the Brain Stimulation Practitioner. Neuromodulation. 2022;25(8):1289-98. 10.1016/j.neurom.2021.09.003. 58. Brown JC, Yuan S, DeVries WH, Armstrong NM, Korte JE, Sahlem GL, et al. NMDA- receptor agonist reveals LTP-like properties of 10-Hz rTMS in the human motor cortex. Brain Stimul. 2021;14(3):619-21. 10.1016/j.brs.2021.03.016. 59. Lu B, Nagappan G, Lu Y. BDNF and synaptic plasticity, cognitive function, and dysfunction. Handb Exp Pharmacol. 2014;220:223-50. 10.1007/978-3-642-45106-5_9. 60. Ma J, Zhang Z, Su Y, Kang L, Geng D, Wang Y, et al. Magnetic stimulation modulates structural synaptic plasticity and regulates BDNF-TrkB signal pathway in cultured hippocampal neurons. Neurochem Int. 2013;62(1):84-91. 10.1016/j.neuint.2012.11.010. 61. Lu Y, Christian K, Lu B. BDNF: a key regulator for protein synthesis-dependent LTP and long-term memory? Neurobiol Learn Mem. 2008;89(3):312-23. 10.1016/j.nlm.2007.08.018. 62. Wu Y, Shao W, Todd TW, Tong J, Yue M, Koga S, et al. Microglial lysosome dysfunction contributes to white matter pathology and TDP-43 proteinopathy in GRN-associated FTD. Cell Rep. 2021;36(8):109581. 10.1016/j.celrep.2021.109581. 63. Zhu H, Yan H, Tang N, Li X, Pang P, Li H, et al. Impairments of spatial memory in an Alzheimer's disease model via degeneration of hippocampal cholinergic synapses. Nat Commun. 2017;8(1):1676. 10.1038/s41467-017-01943-0.
View at Publisher | View at Google Scholar - Present, and Future of a Globally Progressive Disease. Cureus. 2024;16(1):e51705. 10.7759/cureus.51705.
View at Publisher | View at Google Scholar - van Dyck CH, Swanson CJ, Aisen P, Bateman RJ, Chen C, Gee M, et al. Lecanemab in Early
View at Publisher | View at Google Scholar - Alzheimer's Disease. N Engl J Med. 2023;388(1):9-21. 10.1056/NEJMoa2212948.
View at Publisher | View at Google Scholar - Sims JR, Zimmer JA, Evans CD, Lu M, Ardayfio P, Sparks J, et al. Donanemab in Early
View at Publisher | View at Google Scholar - Symptomatic Alzheimer Disease: The TRAILBLAZER-ALZ 2 Randomized Clinical Trial. Jama.
View at Publisher | View at Google Scholar - 4692023;330(6):512-27. 10.1001/jama.2023.13239.
View at Publisher | View at Google Scholar - 4. Cummings J, Zhou Y, Lee G, Zhong K, Fonseca J, Cheng F. [Not Available]. Alzheimers Dement (N Y). 2024;10(2):e12465. 10.1002/trc2.12465.
View at Publisher | View at Google Scholar - 5. Cole E, O'Sullivan SJ, Tik M, Williams NR. Accelerated Theta Burst Stimulation: Safety,
View at Publisher | View at Google Scholar - Efficacy, and Future Advancements. Biol Psychiatry. 2024;95(6):523-35 10.1016/j.biopsych.2023.12.004.
View at Publisher | View at Google Scholar - 6. Huang YZ, Edwards MJ, Rounis E, Bhatia KP, Rothwell JC. Theta burst stimulation of the
View at Publisher | View at Google Scholar - human motor cortex. Neuron. 2005;45(2):201-6. 10.1016/j.neuron.2004.12.033.
View at Publisher | View at Google Scholar - 7. Yamaguchi T, Fujiwara T, Lin SC, Takahashi Y, Hatori K, Liu M, et al. Priming With Intermittent Theta Burst Transcranial Magnetic Stimulation Promotes Spinal Plasticity Induced by Peripheral Patterned Electrical Stimulation. Front Neurosci. 2018;12:508.10.3389/fnins.2018.00508.
View at Publisher | View at Google Scholar - 8. Gamboa OL, Antal A, Moliadze V, Paulus W. Simply longer is not better: reversal of theta burst after-effect with prolonged stimulation. Exp Brain Res. 2010;204(2):181-7.10.1007/s00221-010-2293-4.
View at Publisher | View at Google Scholar - 9. Huang YZ, Chen RS, Rothwell JC, Wen HY. The after-effect of human theta burst stimulation is NMDA receptor dependent. Clin Neurophysiol. 2007;118(5):1028-32.10.1016/j.clinph.2007.01.021.
View at Publisher | View at Google Scholar - 10. Cohen SL, Bikson M, Badran BW, George MS. A visual and narrative timeline of US FDA milestones for Transcranial Magnetic Stimulation (TMS) devices. Brain Stimul. 2022;15(1):73-5. 10.1016/j.brs.2021.11.010.
View at Publisher | View at Google Scholar - 11. Rounis E, Huang YZ. Theta burst stimulation in humans: a need for better understanding effects of brain stimulation in health and disease. Exp Brain Res. 2020;238(7-8):1707-14.10.1007/s00221-020-05880-1.
View at Publisher | View at Google Scholar - 12. Sharbafshaaer M, Cirillo G, Esposito F, Tedeschi G, Trojsi F. Harnessing Brain Plasticity: The Therapeutic Power of Repetitive Transcranial Magnetic Stimulation (rTMS) and Theta Burst Stimulation (TBS) in Neurotransmitter Modulation, Receptor Dynamics, and Neuroimaging for Neurological Innovations. Biomedicines. 2024;12(11). 10.3390/biomedicines12112506.
View at Publisher | View at Google Scholar - 13. Dragon K, Janthur C, Hebel T, Abdelnaim MA, Reißmann A, Langguth B, et al. Four weeks standard vs. one week accelerated intermittent Theta Burst Stimulation for the treatment of depression – A retrospective analysis. Behavioural Brain Research. 2025;479:115361. https://doi.org/10.1016/j.bbr.2024.115361.
View at Publisher | View at Google Scholar - 14. Zhang M, Li W, Hu Z, Lu H, Zhou Y, Ning Y. Antidepressant response time across intermittent theta burst stimulation regimens and efficacy indicators in adolescents depression: a secondary analysis from a randomized controlled trial. BMC Psychiatry. 2024;24(1):905. 10.1186/s12888-024-06346-2.
View at Publisher | View at Google Scholar - 15. Yu F, Tang X, Hu R, Liang S, Wang W, Tian S, et al. The After-Effect of Accelerated Intermittent Theta Burst Stimulation at Different Session Intervals. Front Neurosci. 2020;14:576. 10.3389/fnins.2020.00576.
View at Publisher | View at Google Scholar - 16. Hodkinson DJ, Drabek MM, Horvath S, Pszczolkowski S, Tench C, Tanasescu R, et al.
View at Publisher | View at Google Scholar - Accelerated intermittent theta burst transcranial magnetic stimulation of the dorsolateral prefrontal cortex for chronic knee osteoarthritis pain. Clin Neurophysiol. 2025.10.1016/j.clinph.2025.02.267.
View at Publisher | View at Google Scholar - 17. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. 2021;372:n71. 10.1136/bmj.n71.
View at Publisher | View at Google Scholar - 18. Varma AR, Snowden JS, Lloyd JJ, Talbot PR, Mann DM, Neary D. Evaluation of the NINCDS-ADRDA criteria in the differentiation of Alzheimer's disease and frontotemporal dementia. J Neurol Neurosurg Psychiatry. 1999;66(2):184-8. 10.1136/jnnp.66.2.184.
View at Publisher | View at Google Scholar - 19. Martorana A, Esposito Z, Di Lorenzo F, Giacobbe V, Sancesario GM, Bucchi G, et al. Cerebrospinal fluid levels of Aβ42 relationship with cholinergic cortical activity in Alzheimer's disease patients. J Neural Transm (Vienna). 2012;119(7):771-8. 10.1007/s00702-012-0780-4.
View at Publisher | View at Google Scholar - 20. McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Jr., Kawas CH, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7(3):263-9. 10.1016/j.jalz.2011.03.005.
View at Publisher | View at Google Scholar - 21. McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology. 1984;34(7):939-44. 10.1212/wnl.34.7.939.
View at Publisher | View at Google Scholar - 22. Jack CR, Jr., Albert MS, Knopman DS, McKhann GM, Sperling RA, Carrillo MC, et al. Introduction to the recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement.2011;7(3):257-62. 10.1016/j.jalz.2011.03.004.
View at Publisher | View at Google Scholar - 23. Barker TH SJ, Sears K, Klugar M, Tufanaru C, Leonardi-Bee J, Aromataris E, Munn Z. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evidence Synthesis. 2023;21(3):494-506.
View at Publisher | View at Google Scholar - 24. Barker TH HN, Aromataris E, Stone JC, Leonardi-Bee J, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias quasi-experimental studies. JBI Evid Synth 2024;22(3):378-88.
View at Publisher | View at Google Scholar - 25. Hooijmans CR, Rovers MM, de Vries RBM, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLE’s risk of bias tool for animal studies. BMC Medical Research Methodology. 2014;14(1):43. 10.1186/1471-2288-14-43.
View at Publisher | View at Google Scholar - 26. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. Bmj. 2011;343:d5928.10.1136/bmj.d5928.
View at Publisher | View at Google Scholar - 27. Zhu Y, Huang H, Chen Z, Tao Y, Liao LY, Gao SH, et al. Intermittent Theta Burst Stimulation Attenuates Cognitive Deficits and Alzheimer's Disease-Type Pathologies via ISCA1-Mediated Mitochondrial Modulation in APP/PS1 Mice. Neurosci Bull. 2024;40(2):182-200.10.1007/s12264-023-01098-7.
View at Publisher | View at Google Scholar - 28. Wu C, Lin T, Ding Q, Zhang N, Ou ZT, Cai GY, et al. Continuous Theta-Burst Stimulation Promotes Paravascular CSF-Interstitial Fluid Exchange through Regulation of Aquaporin-4 Polarization in APP/PS1 Mice. Mediators Inflamm. 2022;2022:2140524. 10.1155/2022/2140524.
View at Publisher | View at Google Scholar - 29. Stanojevic JB, Zeljkovic M, Dragic M, Stojanovic IR, Ilic TV, Stevanovic ID, et al. Intermittent theta burst stimulation attenuates oxidative stress and reactive astrogliosis in the streptozotocin-induced model of Alzheimer's disease-like pathology. Front Aging Neurosci.2023;15:1161678. 10.3389/fnagi.2023.1161678.
View at Publisher | View at Google Scholar - 30. Huang H, Zhu Y, Liao L, Gao S, Tao Y, Fang X, et al. The long-term effects of intermittent theta burst stimulation on Alzheimer's disease-type pathologies in APP/PS1 mice. Brain Res Bull. 2023;202:110735. 10.1016/j.brainresbull.2023.110735.
View at Publisher | View at Google Scholar - 31. Stanojevic J, Dragic M, Stevanovic I, Ilic T, Stojanovic I, Zeljkovic M, et al. Intermittent theta burst stimulation ameliorates cognitive impairment and hippocampal gliosis in the Streptozotocin-induced model of Alzheimer's disease. Behav Brain Res. 2022;433:113984.10.1016/j.bbr.2022.113984.
View at Publisher | View at Google Scholar - 32. Stekic A, Zeljkovic M, Zaric Kontic M, Mihajlovic K, Adzic M, Stevanovic I, et al. Intermittent Theta Burst Stimulation Ameliorates Cognitive Deficit and Attenuates Neuroinflammation via PI3K/Akt/mTOR Signaling Pathway in Alzheimer's-Like Disease Model. Front Aging Neurosci. 2022;14:889983. 10.3389/fnagi.2022.889983.
View at Publisher | View at Google Scholar - 33. Wu X, Yan Y, Hu P, Wang L, Wu Y, Wu P, et al. Effects of a periodic intermittent theta burst stimulation in Alzheimer's disease. Gen Psychiatr. 2024;37(1):e101106. 10.1136/gpsych-2023-101106.
View at Publisher | View at Google Scholar - 34. Wu X, Ji GJ, Geng Z, Wang L, Yan Y, Wu Y, et al. Accelerated intermittent theta-burst stimulation broadly ameliorates symptoms and cognition in Alzheimer's disease: A randomized controlled trial. Brain Stimul. 2022;15(1):35-45. 10.1016/j.brs.2021.11.007.
View at Publisher | View at Google Scholar - 35. Wu X, Ji G-J, Geng Z, Zhou S, Yan Y, Wei L, et al. Strengthened theta-burst transcranial magnetic stimulation as an adjunctive treatment for Alzheimer’s disease: An open-label pilot study. Brain Stimulation: Basic, Translational, and Clinical Research in Neuromodulation.2020;13(2):484-6. 10.1016/j.brs.2019.12.020.
View at Publisher | View at Google Scholar - 36. Lin H, Liang J, Wang Q, Shao Y, Song P, Li S, et al. Effects of accelerated intermittent theta- burst stimulation in modulating brain of Alzheimer's disease. Cereb Cortex. 2024;34(3).10.1093/cercor/bhae106.
View at Publisher | View at Google Scholar - 37. Jin X, Xu CY, Fei JF, Fang Y, Sun CH. Alzheimer's disease with depressive symptoms: Clinical effect of intermittent theta burst stimulation repetitive transcranial magnetic stimulation. World J Psychiatry. 2024;14(8):1216-23. 10.5498/wjp.v14.i8.1216.
View at Publisher | View at Google Scholar - 38. Golaszewski S, Kunz A, Schwenker K, Sebastianelli L, Versace V, Ferrazzoli D, et al. Effects of Intermittent Theta Burst Stimulation on the Clock Drawing Test Performances in Patients with Alzheimer's Disease. Brain Topogr. 2021;34(4):461-6. 10.1007/s10548-021-00836-2.
View at Publisher | View at Google Scholar - 39. Olğun Y, Aksoy Poyraz C, Bozluolçay M, Gündüz A, Poyraz B. A comparative transcranial magnetic stimulation study: Assessing cortical excitability and plasticity in Alzheimer's disease, dementia with Lewy bodies and Frontotemporal dementia. Psychogeriatrics. 2024;24(2):272-80.10.1111/psyg.13070.
View at Publisher | View at Google Scholar - 40. Xiao G, Wu Y, Yan Y, Gao L, Geng Z, Qiu B, et al. Optimized Magnetic Stimulation Induced Hypoconnectivity Within the Executive Control Network Yields Cognition Improvements in Alzheimer's Patients. Front Aging Neurosci. 2022;14:847223. 10.3389/fnagi.2022.847223.
View at Publisher | View at Google Scholar - 41. Di Lorenzo F, Bonni S, Picazio S, Motta C, Caltagirone C, Martorana A, et al. Effects of Cerebellar Theta Burst Stimulation on Contralateral Motor Cortex Excitability in Patients with Alzheimer's Disease. Brain Topogr. 2020;33(5):613-7. 10.1007/s10548-020-00781-6.
View at Publisher | View at Google Scholar - 42. Di Lorenzo F, Martorana A, Ponzo V, Bonni S, D'Angelo E, Caltagirone C, et al. Cerebellar theta burst stimulation modulates short latency afferent inhibition in Alzheimer's disease patients. Front Aging Neurosci. 2013;5:2. 10.3389/fnagi.2013.00002.
View at Publisher | View at Google Scholar - 43. Leblhuber F, Geisler S, Ehrlich D, Steiner K, Kurz K, Fuchs D. High Frequency Repetitive Transcranial Magnetic Stimulation Improves Cognitive Performance Parameters in Patients with Alzheimer's Disease - An Exploratory Pilot Study. Curr Alzheimer Res. 2022;19(9):681-8.10.2174/1567205019666220920090919.
View at Publisher | View at Google Scholar - 44. Hoy KE, Emonson MRL, Bailey NW, Rogers C, Coyle H, Stockman F, et al. Gamma connectivity predicts response to intermittent theta burst stimulation in Alzheimer's disease: a randomized controlled trial. Neurobiol Aging. 2023;132:13-23.10.1016/j.neurobiolaging.2023.08.006.
View at Publisher | View at Google Scholar - 45. Kashyap B, Hanson LR, Gustafson SK, Barclay T, Howe CM, Sherman SJ, et al. Open label pilot of personalized, neuroimaging-guided theta burst stimulation in early-stage Alzheimer's disease. Front Neurosci. 2024;18:1492428. 10.3389/fnins.2024.1492428.
View at Publisher | View at Google Scholar - 46. Fried PJ, Jannati A, Davila-Perez P, Pascual-Leone A. Reproducibility of Single-Pulse, Paired-Pulse, and Intermittent Theta-Burst TMS Measures in Healthy Aging, Type-2 Diabetes, and Alzheimer's Disease. Front Aging Neurosci. 2017;9:263. 10.3389/fnagi.2017.00263.
View at Publisher | View at Google Scholar - 47. Wu X, Ji GJ, Geng Z, Zhou S, Yan Y, Wei L, et al. Strengthened theta-burst transcranial magnetic stimulation as an adjunctive treatment for Alzheimer's disease: An open-label pilot study. Brain Stimul. 2020;13(2):484-6. 10.1016/j.brs.2019.12.020.
View at Publisher | View at Google Scholar - 48. Chu M, Zhang Y, Chen J, Chen W, Hong Z, Zhang Y, et al. Efficacy of Intermittent Theta- Burst Stimulation and Transcranial Direct Current Stimulation in Treatment of Post-Stroke Cognitive Impairment. J Integr Neurosci. 2022;21(5):130. 10.31083/j.jin2105130.
View at Publisher | View at Google Scholar - 49. Alkhasli I, Sakreida K, Mottaghy FM, Binkofski F. Modulation of Fronto-Striatal Functional Connectivity Using Transcranial Magnetic Stimulation. Front Hum Neurosci. 2019;13:190.10.3389/fnhum.2019.00190.
View at Publisher | View at Google Scholar - 50. Toniolo S, Serra L, Olivito G, Marra C, Bozzali M, Cercignani M. Patterns of Cerebellar Gray Matter Atrophy Across Alzheimer's Disease Progression. Front Cell Neurosci. 2018;12:430.10.3389/fncel.2018.00430.
View at Publisher | View at Google Scholar - 51. Toniolo S, Serra L, Olivito G, Caltagirone C, Mercuri NB, Marra C, et al. Cerebellar White Matter Disruption in Alzheimer's Disease Patients: A Diffusion Tensor Imaging Study. J Alzheimers Dis. 2020;74(2):615-24. 10.3233/jad-191125.
View at Publisher | View at Google Scholar - 52. Evans GJ. Synaptic signalling in cerebellar plasticity. Biol Cell. 2007;99(7):363-78.10.1042/bc20070010.
View at Publisher | View at Google Scholar - 53. Koch G, Mori F, Marconi B, Codecà C, Pecchioli C, Salerno S, et al. Changes in intracortical circuits of the human motor cortex following theta burst stimulation of the lateral cerebellum. Clin Neurophysiol. 2008;119(11):2559-69. 10.1016/j.clinph.2008.08.008.
View at Publisher | View at Google Scholar - 54. Wu T, Hallett M. The cerebellum in Parkinson's disease. Brain. 2013;136(Pt 3):696-709.10.1093/brain/aws360.
View at Publisher | View at Google Scholar - 55. Daskalakis ZJ, Paradiso GO, Christensen BK, Fitzgerald PB, Gunraj C, Chen R. Exploring the connectivity between the cerebellum and motor cortex in humans. J Physiol. 2004;557(Pt2):689-700. 10.1113/jphysiol.2003.059808.
View at Publisher | View at Google Scholar - 56. Dum RP, Strick PL. An unfolded map of the cerebellar dentate nucleus and its projections to the cerebral cortex. J Neurophysiol. 2003;89(1):634-9. 10.1152/jn.00626.2002.
View at Publisher | View at Google Scholar - 57. Brown JC, Higgins ES, George MS. Synaptic Plasticity 101: The Story of the AMPA Receptor for the Brain Stimulation Practitioner. Neuromodulation. 2022;25(8):1289-98. 10.1016/j.neurom.2021.09.003.
View at Publisher | View at Google Scholar - 58. Brown JC, Yuan S, DeVries WH, Armstrong NM, Korte JE, Sahlem GL, et al. NMDA- receptor agonist reveals LTP-like properties of 10-Hz rTMS in the human motor cortex. Brain Stimul. 2021;14(3):619-21. 10.1016/j.brs.2021.03.016.
View at Publisher | View at Google Scholar - 59. Lu B, Nagappan G, Lu Y. BDNF and synaptic plasticity, cognitive function, and dysfunction. Handb Exp Pharmacol. 2014;220:223-50. 10.1007/978-3-642-45106-5_9.
View at Publisher | View at Google Scholar - 60. Ma J, Zhang Z, Su Y, Kang L, Geng D, Wang Y, et al. Magnetic stimulation modulates structural synaptic plasticity and regulates BDNF-TrkB signal pathway in cultured hippocampal neurons. Neurochem Int. 2013;62(1):84-91. 10.1016/j.neuint.2012.11.010.
View at Publisher | View at Google Scholar - 61. Lu Y, Christian K, Lu B. BDNF: a key regulator for protein synthesis-dependent LTP and long-term memory? Neurobiol Learn Mem. 2008;89(3):312-23. 10.1016/j.nlm.2007.08.018.
View at Publisher | View at Google Scholar - 62. Wu Y, Shao W, Todd TW, Tong J, Yue M, Koga S, et al. Microglial lysosome dysfunction contributes to white matter pathology and TDP-43 proteinopathy in GRN-associated FTD. Cell Rep. 2021;36(8):109581. 10.1016/j.celrep.2021.109581.
View at Publisher | View at Google Scholar - 63. Zhu H, Yan H, Tang N, Li X, Pang P, Li H, et al. Impairments of spatial memory in an Alzheimer's disease model via degeneration of hippocampal cholinergic synapses. Nat Commun. 2017;8(1):1676. 10.1038/s41467-017-01943-0.
View at Publisher | View at Google Scholar
