

Case Report | DOI: https://doi.org/10.31579/2834-796X/017
A Review of the use of Inferior Vena Cava Filters for the Prevention of Pumulmonary Embolism
- Sotonye T Dodiyi-Manuel
- Emmanuel Auchi Edafe *
University of Port Harcourt Teaching Hospital, Port Harcourt.
*Corresponding Author: Emmanuel Auchi Edafe, University of Port Harcourt Teaching Hospital, Port Harcourt.
Citation: Sotonye T Dodiyi-Manuel., Emmanuel Auchi Edafe., (2023), A Review of the use of Inferior Vena Cava Filters for the Prevention of Pumulmonary Embolism, International Journal of Cardiovascular Medicine, 2(1); DOI:10.31579/2834-796X/017
Copyright: © 2023, Emmanuel Auchi Edafe. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 February 2023 | Accepted: 24 February 2023 | Published: 28 February 2023
Keywords: IVC filters; indication; contra-indication; procedure
Abstract
The management of patients with venous thromboembolism (VTE) is very tasking and may involve a multi-disciplinary approach. The main treatment modality for VTE still remains anticoagulation. There are situations in which anticoagulation may not be sufficient or is contraindicated. The placement of filter devices in the inferior vena cava (IVC) to prevent embolization of deep venous thrombosis (DVT), a well-established secondary treatment option thus becomes necessary. This review discusses, we discuss the indications, contraindications and commonly used filters in the inferior vena cava.
Introduction
Pulmonary embolism (PE) is a cause of significant morbidity and mortality in both low- and high-income countries of the world. [1] It is estimated to be among the leading cardiovascular causes of mortality, with an estimated 3-month mortality rate ranging from 15% to 18%.[1] When PE is not treated properly, it may lead to chronic pulmonary hypertension and right heart strain. A major source of PE is deep venous thrombosis that is formed in the lower limbs and pelvic veins. [1] Once the diagnosis of deep vein thrombosis (DVT) is made, urgent treatment with anticoagulation is paramount to prevent severe and life-threatening complications such as PE and the post-thrombotic state (pain, heaviness, leg swelling, and ulceration).[2] Medical remedies for DVT include low-molecular-weight heparin, unfractionated heparin and oral anticoagulants such as vitamin K and non-vitamin K antagonists. [2] In situations where anticoagulation is not feasible or is shown to be ineffective, inferior vena cava (IVC) filters may be used to prevent pulmonary embolism.
The implantable IVC filter was first introduced by Mobin-Uddin in 1969 and Greenfield in 1973, and the use of IVC filters has grown tremendously since the 1990s. [3] An IVC filter is a metallic filter placed endovascularly into the IVC to prevent lower extremity blood clots from embolizing to the right side of the heart and the pulmonary arterial circulation. Blood clots that are trapped in the IVC filter are then dissolved by the body’s own natural thrombolytic mechanisms. [4] Retrievable IVC filters are those that may be removed percutaneously or may be left in place permanently. Permanent IVC filters stay in place and are not removed. Permanent filters are rarely indicated nowadays. Most filters implanted nowadays are the temporary filters which can be removed when the indication for use ceases.
A retrievable IVC filter can be removed by capturing the hook on the IVC filter tip with a snare and removing the filter through a sheath. This radiopaque hook may often be seen on plain radiographs to determine whether the IVC filter is the type that may be retrievable or is better left. Other integral components of an IVC filter include the tip and the arms (shorter struts) and legs (longer struts). The tip of the filter should always point in the direction of blood flow toward the heart so that clots may be captured within the filter legs. The objective of this review is to evaluate the techniques and indications for the IVC filters which would be beneficial especially in low- and middle-income countries.
Characteristics of ideal IVC filters.5
The features of ideal IVC filters include the following: [5] 1. Non-thrombogenic, biocompatible, long-life material, 2. High filtering efficiency for large and small emboli without impedance of flow. 3. Secure fixation within the vena cava. 4. Rapid percutaneous insertion with good release mechanism simple and controlled and amenable to repositioning. 5. MR imaging compatibility e.g., nonferromagnetic. 6. Low cost 8. Retrievability should be easy and very simple.
There is however no filter that meets all the above criteria up till date. [5]
Commonly placed IVC filters.[6] The table 1 below shows the commonly used IVC filters worldwide. The various sizes are shown.
In Nigeria, the commonly used IVC filter is ALN filters. The reason may be due to cost.
Name | Manufacturer | MRI compatibility | Permanent/Retrievable | Approved caval diameter (mm) |
ALN vena cava filter | ALN | Conditional to 3T | Yes | 32 |
OptionElite | Argon | Conditional to 3T | Yes | 30 |
Denali | Bard | Conditional to 3T | Yes | 28 |
Recovery G2 | Bard | Conditional to 3T | Yes | 28 |
Sentry | Boston Scientific | Conditional to 3T | No (Bio convertible) | 28 |
Greenfield | Boston Scientific | Safe to 1.5T | No | 28 |
VenaTech LP | B.Braun | Conditional to 3T | No | 28 |
VenaTech | B.Braun | Conditional to 3T | No (Convertible) | 28 |
Celect | Cook | Conditional to 3T | Yes | 30 |
Gunther Tulip | Cook | Conditional to 3T | Yes | 30 |
Bird’s Nest | Cook | Conditional to 3T | No | 40 |
OptEase | Cordis | Conditional to 3T | Yes | 40 |
Table 1: Commonly used IVC filters
Indications for Use of Ivc Filters
There are many indications for the use of IVC filters, however, only a few are recommended in the guidelines. The Society of Interventional Radiology (SIR) published guidelines in 2020 in collaboration with the American College of Cardiology, American College of Chest Physicians, American College of Surgeons Committee on Trauma, American Heart Association, Society for Vascular Surgery (SVS), and Society for Vascular Medicine (SVM) in the Treatment of Patients with Venous Thromboembolic Disease recommend the following: [7]
1. In patients with acute pulmonary embolism, with a contraindication to anticoagulation therapy, the use of IVC filter be considered based on various clinical risk factors. [the strength of recommendation: Limited]
2. In patients with acute DVT without PE and with a contraindication to anticoagulation therapy, an IVC filter could be considered based on various clinical risk factors. [Strength of recommendation: Consensus]
3a. In patients undergoing anticoagulation for acute VTE (DVT, PE) in whom a contraindication to anticoagulation develops, an IVC filter be considered in the setting of ongoing significant clinical risk for PE. The Strength of recommendation is Consensus.
3b. In patients undergoing extended anticoagulation for VTE (DVT, PE) and have completed the acute phase of treatment in whom a contraindication to anticoagulation develops, an IVC filter should not be placed, with rare exceptions. The Strength of recommendation is Consensus
4. In patients who are receiving therapeutic anticoagulation for VTE (DVT, PE) who experience a recurrent VTE, we suggest that a filter not be placed, with few exceptions. Reasons for anticoagulation failure should always be addressed. The Strength of recommendation: Consensus
5. In patients with acute VTE (DVT, PE) who are being treated with therapeutic anticoagulation, there is recommend against routine placement of an IVC filter. The Strength of recommendation is Moderate.
6. In patients with acute PE who are undergoing advanced therapies, we suggest considering the placement of IVC filters only in select patients. The Strength of recommendation is Limited
DVT with Advanced Therapies.
7. In patients with DVT who are undergoing advanced therapies, suggest to considering the placement of IVC filters only in select patients. The Strength of recommendation: Limited.
8. In trauma patients without known acute VTE, there is a recommendation against the routine placement of IVC filters for primary VTE prophylaxis. The Strength of recommendation is Moderate
9. In patients without known acute VTE who are undergoing major surgery, we suggest against the routine placement of IVC filters. The strength of recommendation is Consensus
10. In patients who have indwelling IVC filters with no other indication for anticoagulation, the recommendation is against anticoagulation. The strength of the recommendation is consensus.
11a. In patients with indwelling retrievable/convertible IVC filters whose risk of PE has been mitigated or who are no longer at risk for PE, there is a suggestion that filters be routinely removed/converted unless the risk outweighs the benefit. The strength of recommendation is consensus
11b. In patients with indwelling permanent IVC filters whose risk of PE has been mitigated or who are no longer at risk for PE, there is a suggestion against routine removal of filters. The strength of recommendation is Consensus.
12. In patients with complications attributed to indwelling IVC filters, there is the suggestion that filter removal be considered after weighing filter- versus procedure-related risks and the likelihood that filter removal will alleviate the complications. The strength of recommendation is consensus.
13. In patients who have an IVC filter, the recommendation is to use structured follow-up program to increase retrieval rates and detect complications. Strength of recommendation is limited.
14. In patients undergoing IVC filter placement, there is recommendation against any specific placement technique.
Typical indication for IVCF placement
The typical indication for placement of an IVC filter is the existence of VTE with an absolute contraindication to anticoagulation, a complication of anticoagulation, or failure of anticoagulation. [8] The advantage of IVC filter insertion in the setting of acute PE is the prevention of morbidity and mortality from hemodynamic effects of PE recurrence. However, limited low-quality observational studies support this practice. [9,10] Routine use of IVC filters is not recommended (Class IIIa evidence) in patients with VTE treated with therapeutic anticoagulation. [7,12] IVC filter placement should be considered when anticoagulation needs to be stopped due to the occurrence of significant bleeding. [12] A cohort study of patients with significant bleeding risk and VTE
Insertion and Retrieval Techniques
IVC filter placement is best for the IVC from the hepatic veins to the level of the iliac vein bifurcation. This can be grouped into infra-renal and supra-renal position. There are two common well established endovascular approaches which are the trans jugular (neck) and transfemoral (groin). [3] The most practiced method is the trans femoral vein route in sub-Saharan Africa. [13] Most of the IVC filter positioned in the region is commonly in the infra-renal vein vein level.
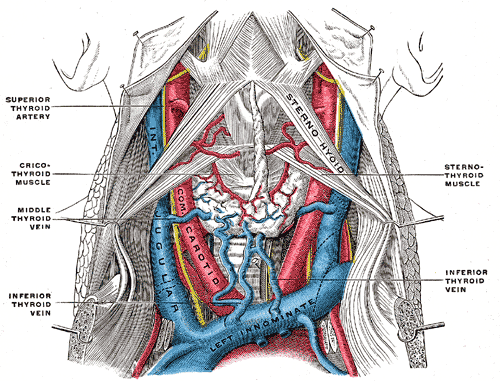
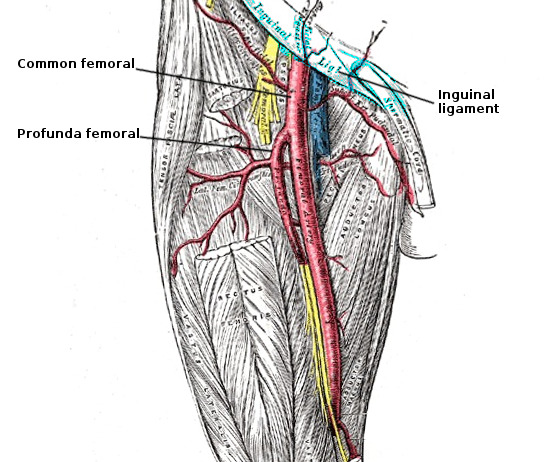
Anatomy
The internal jugular vein (IJV) is located anterior and lateral to the carotid artery. A low puncture increases the risk of pneumothorax, and a high puncture increases the risk of arterial puncture because the artery lies more directly posterior to the vein higher up in the neck. The common femoral vein lies medial to the artery. It is advisable to use ultrasonography (US) during the puncture. In sub-Saharan Africa, where ultrasound is not available in most centers, one may use blind puncture from the femoral using the inguinal ligament and directing the puncture more medial to the most medial femoral artery pulsation as landmarks. The anatomic site of the internal jugular and the femoral veins are demonstrated in figures 1 and 2.
Procedural planning
Filter types
While planning the procedure, it is important to take a decision on the type of filter to be used. There are two different types of IVC filters; permanent (non-retrievable) and temporary (retrievable). [19] Permanent filters cannot be removed or repositioned. Temporary filters (optional filters) can be retrieved or removed. With time, the filter becomes incorporated into the caval wall and may not be removable or surgical techniques may be used to remove it. [20-23]
The implanting physicians are responsible for the ongoing care of patients with retrievable IVC filters and should consider removing the filter as soon as the indication for PE prevention is resolved. [21,22] All physicians involved in the treatment and follow-up of patients receiving IVC filters should consider the risks and benefits of filter removal for each patient; a patient should be referred for IVC filter removal when the risk-benefit profile favors removal and the procedure is feasible in light of the patient’s health status. IVC filter placement is associated with a significant risk of malpractice litigation. [24]
Methods of Insertion. [25-28]
There are two methods of insertion. This is via a jugular or a femoral approach. The jugular approach is referable if an iliofemoral thrombus is present. ALN filters are commonly used in Nigeria. The insertion route is written on the filter either via the jugular or femoral. But their retrieval is via the side with the hook i.e jugular approach. The insertion could be carried out under fluoroscopy guided or ultrasound.
Inferior Vena Cava Filter placement
Explain the procedure to the patient and relations. Get informed consent. Evaluate the patient for contrast allergy. Place the patient on nil per oral (nothing by mouth) for 4-6 hours before the procedure. Clean the skin on the groin or neck with chlorhexidine or povidone-iodine solution depending on the access route. Puncture could be done blindly with palpation of the femoral artery as a guide or the use of an ultrasound device (with a sterile cover) to choose a point on the skin above the vein. Infiltrate 5-10mls of local anesthesia under the access skin.
Using an 18-gauge or micro puncture needle, puncture the anterior wall of the vein and enter the vein. Aspirate venous blood to confirm correct positioning. Evaluate the path of the wire on fluoroscopy to ensure an appropriate venous course. If using a micro puncture kit, convert to 0.035-in. wire.
Advance the 0.035 guide wire into the inferior vena cava (IVC). Advance the catheter into the iliac vein and take the venogram to identify the renal vein. The placement could be infra-renal of supra-renal position. The venogram also helps to measure the following:
1. Patency of the IVC
2. Size of the IVC
3. Ensure that no left-side IVC is present
The next step is to deploy the IVC filter if the venogram accepted. Position the catheter (7F catheter) and remove the dilator. Upload the filter in the 7F catheter and use the dilator to deploy it at the right position. Remove the dilation after deployment and take the final fluoroscopy post-deployment. Then remove the catheter and manually compress for 10 to 20 minutes to ensure no bleeding. Then move the patient to the ward for about 4 hours before discharge from the hospital.
Complications
Immediate Complications
There are several immediate complications that may occur during the procedure. During the initial placement of IVC filters, there is a small chance of mal-positioning where the filter is not placed in the infrarenal IVC.
This may be avoided using a careful deployment technique and a properly performed IVC venogram. In addition, the filter itself may not deploy correctly with all its struts not fully expanded. Other immediate complications include those related to access, such as arterial puncture, with major complications occurring in 11%. [29] There is a small chance of hematoma or bleeding, more commonly in groin access. Access site thrombosis may occur.
Filter Migration and Fracture
Filter migration and fracture are feared long-term complications that may cause serious harm. As venous flow is directed upward toward the heart, fractured elements or the filter itself may embolize more centrally. There have been cases of filter migration to the pulmonary artery and right ventricle, occurring from 0.1 % to 1.25%, with the of risk cardiac tamponade. [30] Struts that fracture and embolize to the cardiac wall and causes perforation are treated with open-heart surgery or percutaneously in select cases. Retrieval of intracardiac filters and fragments or those within the pulmonary arteries are quite challenging and require a complex armamentarium of foreign body retrieval devices. [31]
Filter Strut/Leg Perforations
One of the most common complications seen with IVC filters is penetration and perforation of the struts outside the confines of the IVC wall, occurring in 9%-24% of cases, which may represent a natural progression from IVC wall tenting to frank perforation. [32] Perforated struts may interact with adjacent organs, commonly the aorta, bone, ureter, and bowel. Symptomatic aortic and bowel injuries are unusual but have occurred and required surgical repair. [33] There have been rare case reports of penetrating IVC filters causing aortic pseudoaneurysms, retroperitoneal hemorrhage, hydronephrosis, and pancreatitis. Therefore, as advised by the FDA, retrievable IVC filters should be removed as soon as they are no longer needed to avoid these complications. [34]
Inferior Vena Cava Filter Thrombosis
IVC filter placement has been associated with an increased risk of DVTs and IVC thrombosis. According to the literature, IVC thrombosis occurs in 7.7%-30% of patients with IVC filters. [35] In patients without prior DVTs, new DVT may occur. In these cases, if not contraindicated, oral anticoagulation may be initiated to treat the DVT. If the patient is symptomatic, some centers advocate mechanical thrombectomy. A chronically occluded IVC, seen only in 2% of patients, has undergone angioplasty and stented open in some instances. [36]
The table 2 showed the common complications of IVC filter placement.
Complication | Occurrence rate |
Filter migration and embolization (i.e. >2 cm change from original position) | This occurs in less than 1%.37 More than 90% occur after 30 days. |
Filter fracture | This occurs in 2–10% of filter inserted.38 About 40% risk of fracture at 5.5 years |
IVC perforation: of the filter head or strut >3mm beyond the wall of the IVC or within an adjacent structure | The incidence is about 0–41%.39 About 20% of IVC filter complications reported as IVC perforation.37 |
DVT | Incidence at 2 years is about 21% and at 8 years about 36%.40 |
Filter-related thrombosis | This occurs at a rate of 2–30%.38 |
Table 2: IVC filter insertion complication
Contraindications to the filter insertion
The absolute contraindication for IVC placement is lack of access to the IVC and patient refusal of consent. The relative contraindications may include the following:
1.Deranged coagulation
2.Total thrombosis of the IVC
3.Bacteremia, sepsis, or both
4. Caval diameter less than 15 mm
Conclusion
IVC filters are placed for the prevention of pulmonary embolism in patients with contraindications for anticoagulation or those with clear evidence of failed anticoagulation. The advantage of IVC filter insertion in the setting of acute PE is the prevention of morbidity and mortality from hemodynamic effects of PE recurrence. Complications are low and may arise during filter insertion or months after the procedure.
References
- Goldhaber SZ, Bounameaux H. Pulmonary embolism and deep vein thrombosis. Lancet 2012; 379(9828): 1835-1846.
View at Publisher | View at Google Scholar - Burgazli KM, Atmaca N, Mericliler M, Parahuleva M, Erdogan A, Daebritz SH. Deep vein thrombosis and novel oral anticoagulants: A clinical review. Eur Rev Med Pharma Sci 2013; 17(23): 3123-3131.
View at Publisher | View at Google Scholar - Shin BJ, Beecham Chick JF, Stavropoulos WS. Inferior Vena Cava Filters: Placement and Retrieval. J Radiol Nurs 2015; 34:228-236.
View at Publisher | View at Google Scholar - Sarosiek S, Crowther M, Sloan JM. Indications, complications, and management of inferior vena cava filters: The experience in 952 patients at an academic hospital with a level I trauma center. JAMA Int. Med 2013; 173(7): 513-517.
View at Publisher | View at Google Scholar - Weinberg I, Kaufman J, Jaff MR. Inferior vena cava filters. JACC Cardi Inter 2013; 6(6), 539-547.
View at Publisher | View at Google Scholar - Angel LF, Tapson V, Galgon RE, Restrepo MI, Kaufman J. Systematic review of the use of retrievable inferior vena cava filters. Journal of Vascular and Interventional Radiology 2011; 22: 1522-1530
View at Publisher | View at Google Scholar - Kaufman JA, Barnes GD, Chaer RA, Cuschieri J, Eberhardt RT, Johnson MS, et al. Society of interventional radiology clinical practice guideline for inferior vena cava filters in the treatment of patients with venous thromboembolic disease: developed in collaboration with the american college of cardiology, american college of chest physicians. American College of Surgeons Committee on Trauma, American Heart Association, Society for Vascular Surgery, and Society for Vascular Medicine Journal of Vascular and Interventional Radiology: JVIR 2020; 31: 1529–1544
View at Publisher | View at Google Scholar - DeYoung E, Minocha J. Inferior vena cava filters: guidelines, best practice, and expanding indications. Semin Intervent Radiol 2016; 33: 65–70
View at Publisher | View at Google Scholar - Sarosiek S, Rybin D, Weinberg J, Burke PA, Kasotakis G, Sloan JM. Association between inferior vena cava filter insertion in trauma patients and in-hospital and overall mortality. JAMA Surg 2017; 152: 75–81.
View at Publisher | View at Google Scholar - White RH, Brunson A, Romano PS, Li Z, Wun T. Outcomes after vena cava filter use in noncancer patients with acute venous thromboembolism: A population-based study. Circulation 2016; 133: 2018–2029
View at Publisher | View at Google Scholar - Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing G-J, Harjola V-P, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the european respiratory society (ERS). Eur Heart J 2020; 41: 543–603.
View at Publisher | View at Google Scholar - Muriel A, Jiménez D, Aujesky D, Bertoletti L, Decousus H, Laporte S, et al. Survival effects of inferior vena cava filter in patients with acute symptomatic venous thromboembolism and a significant bleeding risk. J Am Coll Cardiol 2014; 63: S0735-1097(14)01171-1: 1675–1683:
View at Publisher | View at Google Scholar - Edafe EA, Okoro TEO, Stanley KN. Common Indications for IVC Filter Placement in Nigeria: Three Case Series. J Interv Gen Cardiol, 2021, Volume 5(4):1-3.
View at Publisher | View at Google Scholar - Mumtaz S, Singh M. Surgical review of the anatomical variations of the internal jugular vein: an update for head and neck surgeons. Ann R Coll Surg Engl. 2019 Jan;101(1):2-6.
View at Publisher | View at Google Scholar - Kunhahamed MO, Abraham SV, Palatty BU, Krishnan SV, Rajeev PC, Gopinathan V. A Comparison of Internal Jugular Vein Cannulation by Ultrasound-Guided and Anatomical Landmark Technique in Resource-Limited Emergency Department Setting. J Med Ultrasound. 2019 Oct-Dec;27(4):187-191.
View at Publisher | View at Google Scholar - Salazar PA, Blitzer D, Dolejs SC, Parent JJ, Gray BW. Echocardiographic Guidance During Neonatal and Pediatric Jugular Cannulation for ECMO. J Surg Res. 2018 Dec;232:517-523.
View at Publisher | View at Google Scholar - Boese CK, Dargel J, Oppermann J, Eysel P, Scheyerer MJ, Bredow J, Lechler P. The femoral neck-shaft angle on plain radiographs: a systematic review. Skeletal Radiol. 2016 Jan;45(1):19-28
View at Publisher | View at Google Scholar - Carballido-Gamio J, Nicolella DP. Computational anatomy in the study of bone structure. Curr Osteoporos Rep. 2013 Sep;11(3):237-45
View at Publisher | View at Google Scholar - Kinney TB. Update on inferior vena cava filters. J Vasc Interv Radiol. 2003 Apr. 14 (4):425-440
View at Publisher | View at Google Scholar - Smouse HB, Rosenthal D, Thuong VH, Knox MF, Dixon RG, Voorhees WD 3rd, et al. Long-term retrieval success rate profile for the Günther Tulip vena cava filter. J Vasc Interv Radiol. 2009 Jul. 20 (7):871-7; quiz 878.
View at Publisher | View at Google Scholar - Dixon A, Stavropoulos SW. Improving retrieval rates for retrievable inferior vena cava filters. Expert Rev Med Devices. 2013 Jan. 10 (1):135-141.
View at Publisher | View at Google Scholar - Dinglasan LA, Oh JC, Schmitt JE, Trerotola SO, Shlansky-Goldberg RD, Stavropoulos SW. Complicated inferior vena cava filter retrievals: associated factors identified at preretrieval CT. Radiology. 2013 Jan. 266 (1):347-354.
View at Publisher | View at Google Scholar - Simon TE, Walker PF, Daab LJ, White JM, White PW. A quality improvement project to improve inferior vena cava filter retrieval. J Vasc Surg Venous Lymphat Disord. 2017 Jan. 5 (1):42-46
View at Publisher | View at Google Scholar - Phair J, Denesopolis J, Lipsitz EC, Scher L. Inferior Vena Cava Filter Malpractice Litigation: Damned if You Do, Damned if You Don't. Ann Vasc Surg. 2018 Jul. 50:15-20
View at Publisher | View at Google Scholar - Chiou AC. Intravascular ultrasound-guided bedside placement of inferior vena cava filters. Semin Vasc Surg. 2006 Sep. 19 (3):150-154
View at Publisher | View at Google Scholar - Gunn AJ, Iqbal SI, Kalva SP, Walker TG, Ganguli S, Salazar GM, et al. Intravascular ultrasound-guided inferior vena cava filter placement using a single-puncture technique in 99 patients. Vasc Endovascular Surg. 2013 Feb. 47 (2):97-101
View at Publisher | View at Google Scholar - Grullon J, Qato K, Bahroloomi D, Nguyen N, Conway A, Leung TM, et al. Impact of Access Site Choice on Inferior Vena Cava Filter Angulation and Outcomes. J Vasc Surg Venous Lymphat Disord. 2022 Sep 29
View at Publisher | View at Google Scholar - Matthews BD, Joels CS, LeQuire MH. Inferior vena cava filter placement: pre insertion inferior vena cava imaging. Am Surg. 2003 Aug. 69 (8):649-653
View at Publisher | View at Google Scholar - Van Ha, T.G. Complications of inferior vena caval filters. Seminars in Interventional Radiology 2006): 23(2): 150-155.
View at Publisher | View at Google Scholar - Nakamura H, Komatsu T, Nakahara S, Sakai Y, Taguchi I. Percutaneous removal of inferior vena cava filter after migration to pulmonary artery using an 8-Fr multipurpose catheter. Heart Lung Circ 2015; 24(8): e127-129
View at Publisher | View at Google Scholar - Rogers NA, Nguyen L, Minniefield NE, Jessen, ME, de Lemos JA. Fracture and embolization of an inferior vena cava filter strut leading to cardiac tamponade. Circulation 2009; 119(18): 2535-2536.
View at Publisher | View at Google Scholar - Jia Z, Wu A, Tam M, Spain J, McKinney JM, Wang W. Caval penetration by inferior vena cava filters: A systematic literature review of clinical significance and management. Circulation 2015; 132(10): 944-952.
View at Publisher | View at Google Scholar - Sherman CM, Rao SR, Talluri S, Dwivedi AJ, Ankem MK. Inferior vena cava filter penetration into right proximal ureter. Can J Uro 2015; 21(1): 7160-7162.
View at Publisher | View at Google Scholar - Ford ME, Lippert JA, McGraw JK. Symptomatic filter penetration presenting as pancreatitis. J Vas Int Rad 2010; 21(4): 574-576.
View at Publisher | View at Google Scholar - Streiff MB. Vena caval filters: A comprehensive review. Blood 2000; 95(12): 3669-3677.
View at Publisher | View at Google Scholar - Sildiroglu O, Ozer H, Turba UC. Management of the thrombosed filter-bearing inferior vena cava. Sem in Int Rad 2012; 29(1): 57-63.35
View at Publisher | View at Google Scholar - Angel LF, Tapson V, Galgon RE, Restrepo MI, Kaufman J. Systematic review of the use of retrievable inferior vena cava filters. Journal of Vascular and Interventional Radiology 2011; 22: 1522-1530.
View at Publisher | View at Google Scholar - Caplin DM, Nikolic B, Kalva SP, Ganguli S, Saad WEA, Zuckerman DA, et al. Quality improvement guidelines for the performance of inferior vena cava filter placement for the prevention of pulmonary embolism. J Vasc Interv Radiol 2011; 22: 1499–1506
View at Publisher | View at Google Scholar - Zhou D, Spain J, Moon E, Mclennan G, Sands MJ, Wang W. Retrospective review of 120 celect nferior vena cava filter retrievals: experience at a single institution. J Vasc Interv Radiol 2012; 23: S1051- 0443(12)00812-3: 1557–1563
View at Publisher | View at Google Scholar - Decousus H, Leizorovicz A, Parent F, Page Y, Tardy B, Girard P, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. N Engl J Med 1998; 338: 409–416
View at Publisher | View at Google Scholar - Fried HI, Nathan BR, Rowe AS, Zabramski JM, Andaluz N, Bhimraj A, et al. The Insertion and Management of External Ventricular Drains: An Evidence-Based Consensus Statement: A Statement for Healthcare Professionals from the Neurocritical Care Society. Neurocrit Care. 2016 Feb. 24 (1):61-81.
View at Publisher | View at Google Scholar - Stevens SM, Woller SC, Kreuziger LB, Bounameaux H, Doerschug K, Geersing GJ, et al. Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest. 2021 Dec. 160 (6):e545-e608
View at Publisher | View at Google Scholar
