

Review Article | DOI: https://doi.org/10.31579/2835-8465/016
Meniscus Injury and Physiotherapy Rehabilitation
*Corresponding Author: Mohammad Habibur Rahman, Assistant Professor of Physiotherapy, School of Science and Technology, Bangladesh Open University, Gazipur-1705, Bangladesh.
Citation: Waliul Islam, Mohammad H Rahman, Fabiha Alam, Ehsanur Rahman, (2024), Meniscus Injury and Physiotherapy Rehabilitation, Orthopaedics Case Reports, 3(4); DOI: 10.31579/2835-8465/016
Copyright: ©, 2024, Mohammad Habibur Rahman. This is an open-access artic le distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 July 2024 | Accepted: 17 July 2024 | Published: 24 July 2024
Keywords: meniscus surgery, rehabilitation protocol, evidence-based physiotherapy treatment
Abstract
Meniscus plays a vital role in shock absorption and load transmission while walking and other activities. It is also responsible for providing stability to the knee joint, limiting flexion and extension of the knee joint at extreme angles and providing proprioception. The occurrence of meniscus injuries is very high in contact sports. It is more commonly reported by men than female & the ratio is 4:1 in favor of men. The purpose of this guideline is to guide the clinical practice and patients throughout the post-operative rehabilitation phase. In the case of complex injuries, a more conservative approach should be taken to range of motion, wait bearing and progression of rehabilitation. This is an evidence based reviewed study which reviewed a guideline for a clinician after meniscus injury surgery. Exercise therapy is proven to be effective after surgery according to different phases. This guideline contains instruction about intervention and criteria to progress into the next phase of rehabilitation. It also demonstrates guidance about weight bearing in different states of healing. Study recommended starting functional activity such as stair climbing after 9 to 10 weeks and performing exercise to improve good proximal stability. After 3 months, athletes may start early sports activities with precaution and safety to promote proper movement and safe progression to strengthening. More than 6 months to attend a regular sports event and participate in a full practice program.
Introduction
Meniscus tissue is a functionally significant structure for humans as it plays a vital role in shock absorption, stabilization, proprioception, and nutrition. It contains semilunar cartilage. The most commonly injured joint in the body is the knee [11]. The occurrence of meniscus injuries is very high in contact sports like football and rugby. Furthermore, meniscal injury is more common in athletes who participate in sports that require quick changes of direction, such as basketball or volleyball [5].
Despite being an indispensable part of the knee joint, the meniscus has a limited blood supply and is relatively avascular. It is also a helpful structure for maintaining the congruence of the joint surface of the knee [14]. Furthermore, it is also responsible for providing stability to the knee joint, limiting flexion and extension of the knee joint at extreme angles and providing proprioception [10]. The symptoms include pain on joint line, clicking during occurrence, swelling, catching, locking, and felling of giving away of the joint. It is more commonly reported by men than women. The ratio is 4:1 in favor of men [8]. Meniscus injury often present with other condition such as anterior cruciate ligament injury (ACL), posterior cruciate ligament injury (PCL) [17].
A meniscal tear can be classified by the pattern and location of the injury. It is shown in figure 1, that the pattern can be vertical, horizontal, or complex. A vertical tear can be longitudinal, usually involves the peripheral aspect of the meniscus. This pattern is termed as a ‘bucket handle’ lesion, which is not often symptomatic if small. A horizontal lesion may be complete or partial cleavage. A complete cleavage divides the meniscal edge into two parts. Partial cleavage is often seen in “flap tears’’. A complex tear is related to the degeneration of knee joints which have both vertical and horizontal components [3].

Figure 1: type of meniscal tear.
Evidence reported that the injury can be divided into three zones respectively, red-red zone (0 to 3 mm away from meniscosynovial junction), red-white zone (3 to 5 mm away from meniscosynovial junction), and white-white zone (More than 5 mm away from meniscosynovial junction). The healing rate is higher in the red-red zone compare to white-white zone as it has higher blood supply [7].
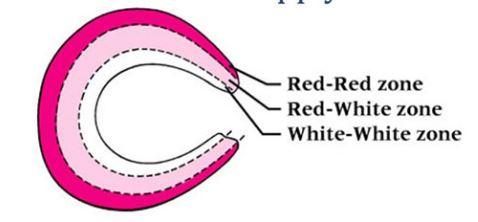
Figure 2: zone of meniscus.
Young athlete mostly suffers from meniscal tear due to excessive application of force but in older athlete it can occur due to normal force due to a degenerative meniscus. Sports related meniscus injury predominantly occurs due to damage during twisting motions, which are common in varus and valgus force directed to a flexed knee. Most common mechanism of traumatic meniscus injury accounting for nearly 50% of injuries, in combination of valgus force directed to knee joint in flexed position [18].

Figure 3: valgus force directed towards flexed knee.
A study reported that clinical examination by expert practitioner provide equal or better outcome than MRI for diagnosis of both medial or lateral meniscus. The study was conducted with 80 patients and they included three physical tests those are McMurray’s test, joint line tenderness test, and Apley's test [1]. The result of that study is shown on table 1 and 2. McMurray's test has sensitivity 79.7%, specificity 78.5%, accuracy 79.4%, a positive likelihood ratio 3.7, a negative likelihood ratio 0.2. Apley's test has a sensitivity 83.7%, a specificity 71.4%, an accuracy 80.3%, a positive likelihood ratio 2.9, negative likelihood ratio 0.2 [22].
| Clinical examination | MRI | |
|---|---|---|
| Sensitivity | 91 | 85 |
| Specificity | 87 | 75 |
| Accuracy | 90 | 82 |
Table 1: Comparison of clinical examination and MRI for medial meniscus injury.
| Clinical examination | MRI | |
|---|---|---|
| Sensitivity | 86 | 85 |
| Specificity | 90 | 91 |
| Accuracy | 87 | 87 |
Table 2: Comparison of clinical examination and MRI for lateral meniscus injury.
Rehabilitation protocol:
This guideline contains clear instruction about intervention and criteria to progress into the next phase of rehabilitation. Interventions are categorized according to duration after surgery. This guideline demonstrates guidance about weight bearing in different states of healing. The goal of this rehabilitation protocol is to protect repair, minimize swelling, reduce pain, restore full extension, muscle inhibition, and educate the athlete about the condition. It can take up to 5 weeks to achieve 120-degree knee flexion. So, in the initial phase, athletes should not flex the knee more than 90 degrees. It is recommended to start functional activity such as stair climbing after 9 to 10 weeks and perform exercise to improve good proximal stability. After 3 months, athletes may start early sports activities with precaution and safety to promote proper movement pattern and safe progression to strengthening. According to protocol, it may take more than 6 months to attend a regular sports event and participate in a full practice program. It is indicated to perform some tests to progress to the next step of rehabilitation, such as a modified stroke test or hop test. If the athlete is unable to meet the criteria to progress to the next phase, he/she needs to continue the rehabilitation in the same phase. Intervention is enlisted in table 3. In the appendix section, an assessment form for functional ability is attached.
The main complicated stage in the rehabilitation protocols are weight-bearing and immobilization periods. According to One study [15] immediate post-operative weight-bearing has no influence over the clinical outcome of isolated meniscus repair.
Phase I (0-3 Weeks after surgery)
Intervention
- To reduce swelling
- Application of ice, gentle massage.
- Ankle pump
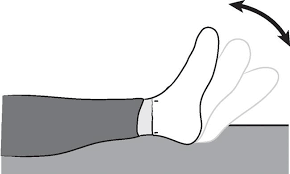
Figure 4: Ankle pump
- Maintain range of motion form mobility.
- Patellar mobilization in all direction.
- Seated assisted knee flexion and heel slides with towel. (Active knee flexion must be avoided in this phase)
- Hamstring stretching in sitting position.
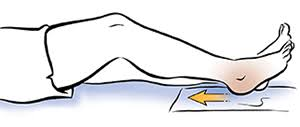
Figure 5: Heel sliding
- Strengthening
- Quadriceps setting exercise.
- Neuro-muscular electrical stimulation (NMES) with high intensity.
- Straight leg raises (have to be avoided in case of leg in knee extension.
- Multi-angle isometric knee extension exercise (with 60-to-90-degree extension)
Phase II (3 to 6 weeks after surgery)
- Range of motion to maintain mobility.
- Stationary bicycle (with in limited range).
- Cardio rehabilitation
- Upper body ergometer

Figure 6: Calf raises
- Strengthening
- Calf raises
- Lumbo-pelvic strength training (sliding of hip external rotation in neutral, plank, bridge with feet elevated)
- Proprioception and balance
- Double limb standing balance utilizing uneven surface using uneven surface.
- Re-tanning of joint position.

Figure 7: Double limb standing balance
- Maintain range of motion
- Supine active hamstring stretching
- Gentle stretching of all muscle group. (Prone quadriceps stretching, standing quadriceps stretching, gastrocnemius stretching, soleus muscle stretching).
- Tibial mobilization (rational) in case of limited range of motion

Figure 8: Supine hamstring stretching
- Cardio
- Stationary bicycle with in available range of motion. Jogging in pool, flutter kick swimming.

Figure 9: Partial squatting exercise
- Strengthening
- Partial squatting exercise (within 0-to-60-degree range of motion)
- Ball squatting, wall sliding (from 0-to-60-degree range of motion)
- Hamstring strength training in prone lying and standing with hamstring curls.
- Bridging with gymnastic ball, hip hiking.
- Progression of exercise with duration and intensity.
- Balance and proprioception
- Balance training with single limb on unstable surface.
Phase IV (9 to 12 weeks after surgery)
● Cardio
• Elliptical, up staring or climbing
● Strengthening
• Squat to chair.
• Lateral lunges
• Single leg progression (partial weight bearing single leg press, slide board lunges: retro and lateral, step ups and step ups with march, lateral step-ups, step downs, single leg squats, single leg wall slides)
• Knee Exercises for additional exercises and descriptions
• Gym equipment (seated hamstring curl machine and hamstring curl machine, Romanian deadlift).
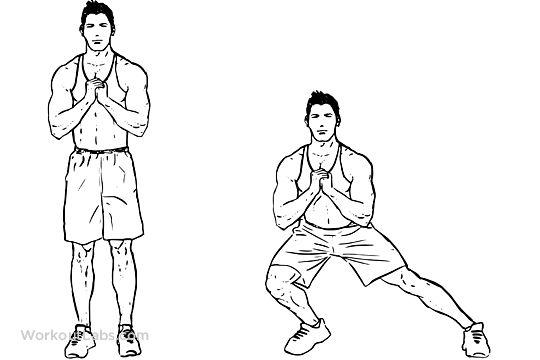
Figure 10: Lateral lunges
Phase V (12 to 20 weeks after surgery)
● Initiation of running with interval
• Return to running activity
● Progress to plyometric and agility program with functional bracing if recommended
• Agility and plyometric exercise.
Figure 11: Plyometric exercise
Phase V (24 weeks after surgery to RTP)
- Multiplan sports specific plyometric program
- Multiple sports specific agility training
- Hard cutting practices
- Non-contact practice to full Practice to full play

Figure 12: Multiple sports specific plyometric and agility training
Guideline for phase progression [19]
Phase I to phase II: Range of motion of knee joint should be 90 degree (flexion) and 0 degree (extension). Athlete has to perform straight leg raise without lagging. Active contraction of quadriceps.
Phase II to phase III: Negative swelling test. Knee flexion up to 120 degrees.
Phase III to phase IV: No after exercise. Normal gait. ROM similar to sound limb. Symmetrical joint sense.
Phase IV to phase V: Hope test equal or greater than 90% compare to sound limb. Completion of jogging, running without pain and swelling
Discussion
A cohort study was done with the aim of identifying characteristics concerning return to the same level of sport and evaluating continuing effects of the injury and management approach on performance. The study was done with recorded data from major European leagues (EPL, Bundesliga, La Liga, Ligue 1 and Serie A) from 2006 to 2016. Two hundred and fifty players were included who matched the inclusion criteria (RTP to the same league, RTP within 2 seasons, field time, and performance metrics). 106 players out of a total of 250 received surgical treatment. of RTP was 70% and, of those, the reinjury rate was 5%. There was no significant difference in field time and performance compared to the control group. But the defender receiving surgical management showed less filed time compared to non-operative management. But in the case of the attacker and midfielder, the field time was the same. Additionally, the players aged more than 30 years demonstrated a negative predictor. Finally, they concluded that elite-level athletes who return to sports following meniscal injury can be expected to perform similarly to before, depending on age, pre-injury performance, and treatment approach [13].
Recently, a retrospective case series was conducted to evaluate the patient's return to sport after meniscal allograft transplantation. Patients who took part in the study underwent allograft transplantation between 2013 and 2015. In addition to patient-reported outcome measures, all patients were surveyed about their return to sports, satisfaction, and subsequent surgery. The most common reasons for participants discontinuing sports were to prevent further damage (more than 70%), pain during activity (more than 50%), fear of further injury (less than 50%), surgeon recommendation (more than 30%), and swelling during activity (thirty percent). They also reported that 75.6% of athletes undergoing arthroscopic transplantation are able to return to at least one sport within one year (+/- 6 months) postoperatively. After transplantation, 48% of patients return to their preoperative activity intensity level. The reoperation rate was 29.9%. 62% were satisfied with their sports participation [23].
Conclusion
In the field of sports injury, meniscal injury is a concerning musculoskeletal pathology. Accurate diagnosis and identifying the degree of injury are very important for the sports clinician as early as possible to prevent further damage and establish a management plan. It is important not to depend on radiological findings but use evidence-based knowledge to analyze the situation clinically based on clinical reasoning principles. For accomplishing a good rehabilitation protocol, it is very significant to know the prognosis and physiology of different stages of the healing process. There are different studies available regarding the anatomy, physiology, and pathology of meniscus injury in databases such as PubMed, Cochrane, Google scholar, and PEDro, etc. It is very important to gather current and up-to-date information regarding those aspects. It is also important to select an appropriate rehabilitation protocol as there are a variety of rehabilitation protocols available. Currently, we are following the general principle of meniscus management, which is also evidence-based. But it is very important for us to develop a conclusive rehabilitation protocol that must be updated on a regular basis for the betterment of the client. So, in this regard, expert practitioners and researchers need to come forward.
References
- Adams, D, Logerstedt, D, Hunter-Giordano, A, Axe, M. J, & Snyder-Mackler, L. (2012). Current concepts for anterior cruciate ligament reconstruction: a criterion-based rehabilitation progression. Journal of orthopedic & sports physical therapy, 42(7), 601-614.
View at Publisher | View at Google Scholar - Brelin, A. M, & Rue, J. P. (2016). Return to play following meniscus surgery. Clin Sports Med, 35(4):669-678.
View at Publisher | View at Google Scholar - Bryceland, J. K., Powell, A. J, & Nunn, T. (2017). Knee menisci: structure, function, and management of pathology. Cartilage, 8(2): 99-104.
View at Publisher | View at Google Scholar - DeFroda, S. F, Bokshan, S. L, Boulos, A, & Owens, B. D. (2018). Variability of online available physical therapy protocols from academic orthopedic surgery programs for arthroscopic meniscus repair. The Physician and Sports medicine, 46(3):355-360.
View at Publisher | View at Google Scholar - DeHaven, K. E, & Bronstein, R. D. (1997). Arthroscopic medial meniscal repair in the athlete. Clinics in sports Medicine, 16(1):69-86.
View at Publisher | View at Google Scholar - Drosos, G. I, &Pozo, J. L. (2004). The causes and mechanisms of meniscal injuries in the sporting and non-sporting environment in an unselected population. The Knee, 11(2), 143-149.
View at Publisher | View at Google Scholar - Eggli, S, Wegmüller, H, Kosina, J, Huckell, C, & Jakob, R. P. (1995). Long-term results of arthroscopic meniscal repair: an analysis of isolated tears. The American journal of sports medicine, 23(6):15-720.
View at Publisher | View at Google Scholar - Englund, M, Guermazi, A, &Lohmander, S. L. (2009). The role of the meniscus in knee osteoarthritis: a cause or consequence. Radiologic Clinics, 47(4):703-712.
View at Publisher | View at Google Scholar - Giuliani, M. J. R., Burns, M. T. C, Svoboda, L. S. J., Cameron, K. L, & Owens, L. B. D. (2011). Treatment of meniscal injuries in young athletes. The journal of knee surgery 24(02), 093-100.
View at Publisher | View at Google Scholar - Greis, P. E., Bardana, D. D., Holmstrom, M. C., & Burks, R. T. (2002). Meniscal injury: I. Basic science and evaluation. JAAOS-Journal of the American Academy of Orthopaedic Surgeons, 10(3), 168-176.
View at Publisher | View at Google Scholar - Higuchi, H, Kimura, M., Shirakura, K, Terauchi, M, &Takagishi, K. (2000). Factors affecting long-term results after arthroscopic partial meniscectomy. Clinical Orthopaedics and Related Research (1976-2007), 377:161-168.
View at Publisher | View at Google Scholar - Kopf, S, Beaufils, P, Hirschmann, M. T, Rotigliano, N, Ollivier, M, Pereira, H, Verdonk, R, Darabos, N, Ntagiopoulos, P, Dejour, D, & Becker, R. (2020). Management of traumatic meniscus tears: the 2019 ESSKA meniscus consensus. Knee Surgery, Sports Traumatology, Arthroscopy, 28(4):1177-1194.
View at Publisher | View at Google Scholar - Lavoie-Gagne, O. Z, Korrapati, A, Retzky, J, Bernstein, D. N, Diaz, C. C, Berlinberg, & Forsythe, B. (2022). Return to Play and Player Performance After Meniscal Tear Among Elite-Level European Soccer Players: A Matched Cohort Analysis of Injuries From 2006 to 2016. OrthopaedicJournal of Sports Medicine, 10(1).
View at Publisher | View at Google Scholar - Matar, H. E., Duckett, S. P., & Raut, V. (2019). Degenerative meniscal tears of the knee: evaluation and management. British Journal of Hospital Medicine, 80(1), 46-50.
View at Publisher | View at Google Scholar - O’Donnell K, Freedman KB, Tjoumakaris FP. Rehabilitation protocols after isolated meniscal repair: a systematic review. The American journal of sports medicine. 2017 Jun;45(7):1687-97.
View at Publisher | View at Google Scholar - Scuderi, G. R, &Tria, A. J. (Eds.). (2010). the knee: a comprehensive review.
View at Publisher | View at Google Scholar - Shiraev, T., Anderson, S. E., & Hope, N. (2012). Meniscal tear: presentation, diagnosis and management. Australian family physician, 41(4):182-187.
View at Publisher | View at Google Scholar - Smet, E. D, Dyck, P. V, Gielen, J, & Vanhoenacker, F. M. (2020). Sports-related meniscal injury. In Imaging of Orthopedic Sports Injuries, 423-448.
View at Publisher | View at Google Scholar - Vanderhaven, K. L., Perkins, C., & Le, M. (2015). Weightbearing versus no weightbearing after meniscus repair. Sports Health, 7(5):399-402.
View at Publisher | View at Google Scholar - Vaquero, J., &Forriol, F. (2016). Meniscus tear surgery and meniscus replacement. Muscles, ligaments and tendons journal, 6(1):71.
View at Publisher | View at Google Scholar - Woodmass, J. M., Johnson, J. D., Wu, I. T, Saris, D. B, Stuart, M. J, &Krych, A. J. (2017). Horizontal cleavage meniscus tear treated with all-inside circumferential compression stitches. Arthroscopy techniques, 6(4):1329-1333.
View at Publisher | View at Google Scholar - Rinonapoli G, Carraro A, Delcogliano A. (2011). The clinical diagnosis of meniscal tear is not easy. Reliability of two clinical meniscal tests and magnetic resonance imaging. International journal of immunopathology and pharmacology.
View at Publisher | View at Google Scholar - Cvetanovich GL, Christian DR, Garcia GH, Liu JN, Redondo ML, Yanke AB, Cole BJ. (2020). Return to sport and patient satisfaction after meniscal allograft transplantation. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 1;36(9):2456-63.
View at Publisher | View at Google Scholar
