

Review Article | DOI: https://doi.org/10.31579/2835-7957/139
Assessment of the Alterations of Semen Parameters after Varicocelectomy among Varicocele Patients in Tripoli, Libya
1Surgery Department, Faculty of Medicine, Sabratha University, Libya
2Pharmacology Department, Faculty of Medicine, Sabratha University, Libya
3Physiology Department, Faculty of Medicine, Sabratha University, Libya
*Corresponding Author: Wade Alwan M Yahya, Surgery Department, Faculty of Medicine, Sabratha University, Libya.
Citation: Wade Alwan M Yahya, Rabia A M Yahya, Karema El. M. Shkal, Azab E. Azab, (2025), Assessment of the Alterations of Semen Parameters after Varicocelectomy among Varicocele Patients in Tripoli, Libya, Clinical Reviews and Case Reports, 4(6); DOI:10.31579/2835-7957/139
Copyright: © 2025, Wade Alwan M Yahya. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 October 2025 | Accepted: 29 October 2025 | Published: 07 November 2025
Keywords: men with varicoceles, varicocelectomy, semen parameters, tripoli, western libya
Abstract
Background: Varicocele is the most common cause of male infertility worldwide and varicocele repair is the world’s most commonly performed male infertility procedure. The presence of a varicocele has been associated with impaired testicular function, often causing abnormalities in semen parameters, including sperm count, motility and morphology, testis size and histology, blood hormone levels and pregnancy rates. The sub inguinal approach of varicocelectomy is one of the common procedures for treating varicocele.
Objectives: The current study aimed to assess the effect of varicocelectomy on the semen parameters after varicocelectomy among men with varicoceles in Tripoli, western Libya.
Methodology: This study included 50 varicocele patients with ages ranging between 23-47 years old. All patients underwent sub inguinal varicocelectomy with testicular artery preservation and were followed up after 3 and 6 months. In all cases at least two semen analyses were obtained pre-varicocelectomy, 3-, and 6-month post-varicocelectomy. All specimens were collected in a clean, wide-mouthed container. The specimens were collected in the laboratory by masturbation after a period of abstinence of 2-3 days.
Results: The results showed that there was significant improvement of the patient’s semen density postoperative after 3 and 6months P-value <0.005. The improvement in sperm concentration, and motility was 58.3%, 54.3%, 52.1% in each of them respectively. correlation between. There is no statistically significant difference was detected between the preoperative semen motility in the normal and subnormal testicular volume P-value >0.05. There was significant improvement of the patient’s semen motility postoperative after 3- and 6-months P-value <0.005.
Conclusion: In conclusion and according to our results, the results showed that an improvement in semen parameters after 3 & 6 months of varicocelectomy. However, further well-designed studies may be needed to consolidate our result.
1.Introduction
Infertility is considered one of the main public health issues, as it affects about 15% of the couples of reproductive ages [1]. The male factor is involved in 40% - 50% of infertility cases [2]. The common cause of male infertility is varicocele, which in a European study was found to affect 16.6% of 7.802 men referred for infertility [3]. A possible reason for linking varicocele with infertility is the fact that it appears 2–3 times more frequently in men that attend infertility clinics, than in men of the general population or of proven fertility [3-6] Varicocele is recognized as clinical problem, since it is very old in the history, and its association with male infertility is well-established [7, 8]. Over centuries, varicocele was important exclusion criterion for military service [9]. The importance of varicocele lies in its common presentation in the general public and infertility clinics, with an overall prevalence rate of 35-40% in men with primary infertility, and 80% in men with secondary infertility [10]. The etiology of varicocele probably multifactorial [11] and its pathophysiology shows us that can decrease fertility by different mechanism sit [12]. The sub inguinal approach of varicocelectomy is one of the common procedures for treating varicocele. It was described by several authors to simple, safe, and a favorable method for ligation of varicocele [13]. The effectiveness of varicocelectomy is still debatable; some of these authors studied the effect of varicocelectomy on semen parameters and reported marked improvement [14]. However, it was not unlit 1952 that, the possible association between varicocele and human sub fertility was formally recognized such recognition was derived from a single case report, of a men diagnosed with maturation arrest by testis biopsy, in which bilateral varicocelectomy resulted in improved sperm count and pregnancy by coitus [15]. Currently, varicocele is the most common cause of male infertility worldwide and varicocele repair is the world’s most commonly performed male infertility procedure [16]. Several studies have shown a significant correlation between varicocele and poor sperm quality. Some show a correlation with all parameters, and others to variety of different parameters only [17].
2. Objectives
The current study aimed to assess the effect of varicocelectomy on the semen parameters after varicocelectomy among men with varicoceles in Tripoli, western Libya.
3. Subjects and Methods
3.1. Patient selection:
50 varicocele patients were included in the present study, which was carried out within the period from June 2024 to February 2024. All patients were recruited from the urology outpatient clinic, a special clinics in Tripoli, Libya.
3.2 Inclusion Criteria:
Patients aged (23-47) years, complaining of primary infertility with abnormal semen analysis scheduled for varicocelectomy.
3.3. Exclusion Criteria:
Cases with secondary varicocele and Azoospermia patients were excluded.
3.4. Semen analysis
In all cases at least two semen analyses were obtained pre-varicocelectomy, 3, and 6 month post-varicocelectomy. All specimens must be collected in a clean, wide-mouthed container. The specimens were collected in the laboratory by masturbation after a period of abstinence of 2-3 days.
Postoperative semen parameters after 3, 6 months were compared to preoperative data. Perioperative changes in semen parameters were compared to preoperative ultrasound findings.
3.6. Statistical Analyses:
Statistical analysis was done by ANOVA- test using SPSS program V.26. The data were expressed as mean ± SD. The P-value less than 0.05 was significant.
4. Results
4.1. Preoperative patient data
This study included 50 patients with a history of infertility for at least 1 year. Patient age ranged from 23 to 47 years, with a mean age of 38.5 + 8.60 years. The duration of infertility ranged from 12 to 24 months with mean 20.21 months (Table 1).
Variables | Mean + SD |
Age (years) | 38.5+ 8.60 |
Duration of infertility in months | 20.21+ 4.63 |
Table 1: Preoperative patient data
4.2 Preoperative and postoperative degree of improvement in patient’s semen density of normal and subnormal testicular volume
Table (2) and figures (1& 2) shows correlation between pre and postoperative semen density after 3,6 months in normal and subnormal testicular volume. There was significant improvement of the patient’s semen density postoperative after 3 and 6 months P-value <0> Parameter Preoperative Mean + SD After 3 months Mean + SD After 6 months Mean + SD F. test P. value Semen Density of Normal testicular volume 6.98 + 0.52 9.85 + 0.95** 12.84 + 1.24**## 15.652 0.001 Semen Density Subnormal testicular volume 6.83 + 0.24 7.14 + 0.76 * 8.97 + 1.13**## 8.352 0.001
Table 2: Preoperative and postoperative degree of improvement in patient’s semen density of normal and subnormal testicular volume
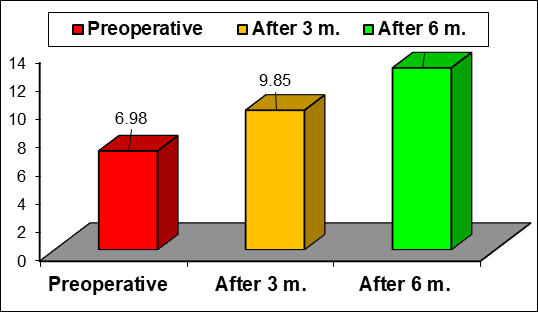
Figure 1: Preoperative and postoperative degree of improvement in patient’s semen density of normal testicular volume
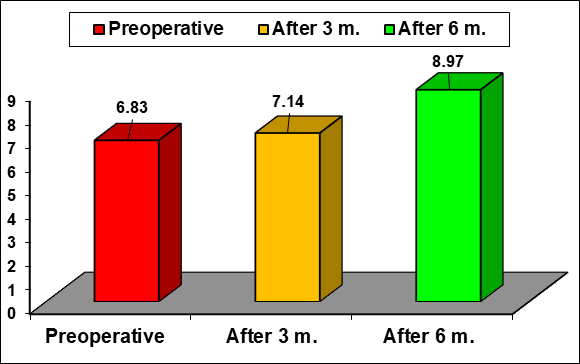
Figure 2: Preoperative and postoperative degree of improvement in patient’s semen density of subnormal testicular volume
4.3. Preoperative semen motility.
Table (3) and figure (3) show correlation between the preoperative semen motility in the normal and subnormal testicular volume. There is no statistically significant difference was detected between two groups P-value >0.05
Parameter | Normal testicular volume Mean + SD | Subnormal testicular volume Mean + SD | F. test | P. value |
Preoperative Semen Motility (%) | 16.5 + 4.53 | 15 + 4.25 | 1.420 | 0.158 |
Table 3: Preoperative semen motility.

Figure 3: Preoperative semen motility (%).
4.5. Preoperative and postoperative degree of improvement in patient’s semen motility in Normal and subnormal testicular volume
Table (4) and figures (4 & 5) shows correlation between pre and postoperative semen motility after 3 & 6 months in normal and subnormal testicular volume. There was significant improvement of the patient’s semen motility postoperative after 3 and 6 months P-value <0> Parameter Preoperative Mean + SD After 3 months Mean + SD After 6 months Mean + SD F. test P. value Semen Motility of Normal testicular volume (%) 16.5 + 4.53 26.75 + 5.86** 33.64 + 8.83**## 8.364 0.001 Semen Motility of Subnormal testicular volume (%) 15 + 4.25 19.50 + 4.95** 26.82 + 7.27**## 7.526 0.001
Table 4: Preoperative and postoperative degree of improvement in patient’s semen motility in Normal and subnormal testicular volume
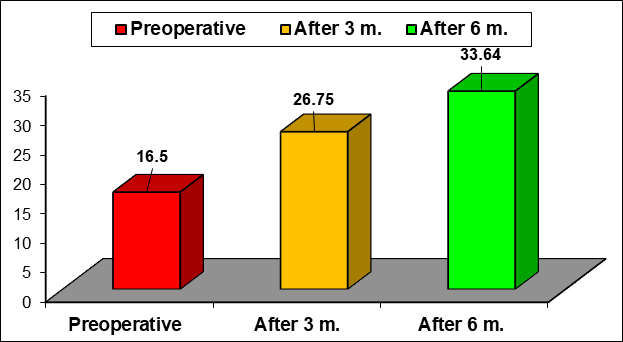
Figure 4: Preoperative and postoperative degree of improvement in patient’s semen motility in Normal testicular volume
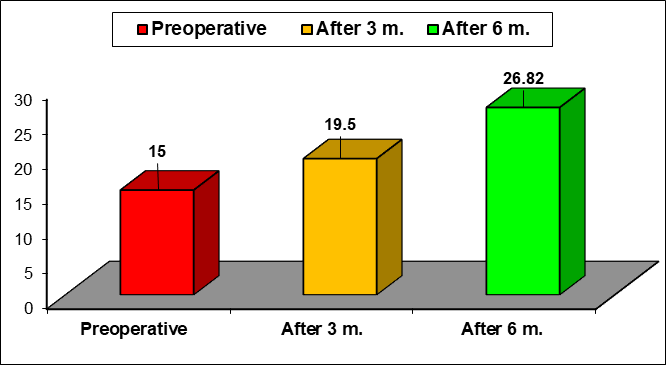
Figure 5: Preoperative and postoperative degree of improvement in patient’s semen motility in subnormal testicular volume
5. Discussion
Varicocele is elongation, dilatation and tortousity of the pampiniform venous plexus and the internal spermatic vein. It is detected in approximately 15–20% of the general male population, with the prevalence increasing to 40% of men with primary infertility, and 80% of men with secondary infertility [18]. The presence of a varicocele has been associated with impaired testicular function, often causing abnormalities in semen parameters, including sperm count, motility and morphology, testis size and histology, blood hormone levels and pregnancy rates [19]. Varicocele is the most common correctable cause in men with infertility. Although, varicocele is also detected in the general population, it is more common in infertile men and treatment can be of benefit for some infertile couples [20]. From June 2024 to February 2025, 50 infertile men with abnormal semen analysis and varicocele were included in the study. Patients with secondary varicocele, 1ry testicular failure and azoospermia were excluded from this study. Also, semen analysis was done preoperative and for follow up after 3 & 6 months. We used improvement index to assess the outcome of varicocelectomy. Improvement index (<0>P< 0>). These results are in agreement with those of Merharban et al. [21]. who found 40.7% and 57.5% improvement index in sperm count and motility, respectively in normal and subnormal testicular volume. Testicular biopsy in males with varicocele shows a wide array of abnormalities. The most common finding are leydig cells hyperplasia, decreased number of the spermatogonia per tubule, spermatogenesis arrest and sloughing of germinal epithelium [22]. A thickened basement membrane of somniferous tubules and proliferative lesions of endothelium are often demonstrated and may affect transportation of oxygen and glucose through these structures [23]. The improvement index was significantly higher in patients with normal testicular volume than in patients with subnormal testicular volume (P< 0>) [24]. Similarly, Pierik et al. [25] found that the increase in sperm count was related positively to testicular volume before surgery.
6. Conclusion
In conclusion and according to our results, the results showed that an improvement in semen parameters after 3 & 6 months of varicocelectomy. However, further well-designed studies may be needed to consolidate our result.
References
- (1999). World Health Organization. Laboratory manual for the examination of human semen and sperm-cervical macus interaction. 4th Ed. New York USA: Cambridge Univeraky Press.
View at Publisher | View at Google Scholar - Speroff L, Glass RH, Kase NG. (1999). Clinical Gynecologic Endocrinology and Infertility. 6th Ed. Baltimore USA: Lippincott Williams & Wilkins; Infertility. pp. 201-246.
View at Publisher | View at Google Scholar - Nieschlag E. (1997). Classification of andrological disorders. In: Nieschlag E, Behre HM, editors. Andrology. Berlin, Heidelberg, New York: Spriger-Verlag. pp. 79-83.
View at Publisher | View at Google Scholar - Papadimas J, Mantalenakis S. (1993). Reproductive Endocrinology in males. Thessaloniki: University Studio Press.
View at Publisher | View at Google Scholar - Saypol DC. (1981). Varicocele. J Androl; 2:61.
View at Publisher | View at Google Scholar - Redmon JB, Carey P, Pryor JL. (2002). Varicocele-the most common cause of male factor infertility? Hum Reprod Update. 8: 53-58.
View at Publisher | View at Google Scholar - Anne M. Jequier, Mele Infertility. (2000). A Guide for the Clinicien by Handcover.
View at Publisher | View at Google Scholar - Dubin 1, Amelar R. (1970). varicocele size and result of varicocelectomy in selected men with varicocele, fertile steril,21: 606-609.
View at Publisher | View at Google Scholar - (2001). Benofa & Gilbert he varicocelt and male infertility part 1, hum sp. Upd.,7: 47-54
View at Publisher | View at Google Scholar - Kamal, K.M., Javeri, K. and Zini, A. (2001). Microsurgical varicocelectomy in the era of assisted reproductive technology, influence of initial semen quality on pregnancy rates. Fertil Steril, 75:1013-1016.
View at Publisher | View at Google Scholar - Skoog sj, Roberts KP, Goldstein m, et al. (1997). the adolescent varicocele: what's new with an old problem in young patients? Pediatrics, 100(1): 112
View at Publisher | View at Google Scholar - Naughton C, Nangia A and agarwa A. (2001). varicocele and male infertility, part II patho physiology of vancocele in male infertility. Human repord update; 71: 473-481.
View at Publisher | View at Google Scholar - Marmar J, kim y. (1994). sub inguinal microsurgical varicocelacionry: a technics) critique and statistical analysis of semen and pregnancy date, J Wol, 152: 1127-1132.
View at Publisher | View at Google Scholar - Yamamoto e, tsuji y and ohuma m. (1995). comparison of artery ligation and artery preserving varicocelectomy effect on postoperative spermatogenesis. Andrologia; 27: 37-40.
View at Publisher | View at Google Scholar - Tulloch w. (1952). a consideration of sterility factors in the light of subooquent pregnancies, sub fertility in male, Edinburgh med; 59: 29-34.
View at Publisher | View at Google Scholar - Khera m & lipshultz: (2005). evolving approach to the varicocele, Aru, Elim, North Am.35: 183-189.
View at Publisher | View at Google Scholar - Hauser, Marc D.; Newport, Elissa L.; Aslin, Richard N. (2001). Segmentation of the speech stream in a non-human primate: Statistical learning in cotton-top tamarins. Cognition, 78.3: B53-B64.
View at Publisher | View at Google Scholar - Kass EJ, and Reitelman C. (1995). Adolescent varicocele. Urol Clin North Am, 1995; 22(1):151-159.
View at Publisher | View at Google Scholar - Nagler HM, Luntz RK, and Martinis FG. Varicocele. In: Lipsbultz LI. et al. (1997). editors. Infertility in the male. St. Louis: Mosby, p. 336-368.
View at Publisher | View at Google Scholar - Madgar I, Weissenberg R, Lunenefeld B. (1995). Controlled trial of high spermatic vein ligation for varicocele in infertile men. Fertil Steril; 63:120-124.
View at Publisher | View at Google Scholar - Mehraban, D., Taghdiri, M., Nategh, S., Ahmadzadeh, A., Ranjbarnovin, N. et al. (2012). Ultrasonic predictors of improved seminal parameters after bilateral laparoscopic varicocelectomy. Inter Urol Nephrol. 44: 1121-1125
View at Publisher | View at Google Scholar - 22.A ragona, F., Ragazzi, R., Pozzan, G. B., De Caro, R., Munari, P. F. et al. (1994). Correlation of testicular volume, histology and Irh test in adolescents with idiopathic varcicocele. Euro urol, 26(1): 61-66
View at Publisher | View at Google Scholar - Hadziselimovic, F., Herzog, B., Liebundgut, B., Jenny, P., & Buser, M. (1989). Testicular and vascular changes in children and adults with varicocele. The Journal of Urology,142(2): 583-585
View at Publisher | View at Google Scholar - Seftel, A. D., Rutchik, S. D., Chen, H., Stovsky, M., Goldfarb, J. et al. (1997). Effects of subinguinal varicocele ligation on sperm concentration, motility and Kruger morphology. The Journal of urology,158(5): 1800-1803.
View at Publisher | View at Google Scholar - Pierik Fil, Vreeburg JT, Stijnen T, et al. (1998). Improvement in sperm count a motilly after ligation of varicoceles detected with color Doppler ultrasonography. Int J Urol; 21(5):256-260.
View at Publisher | View at Google Scholar
